JACARDI as a proof-of-concept for Europe’s Safe Hearts Plan
A new commentary in the International Journal of Public Health explores how JACARDI supports the translation of Europe’s Safe Hearts Plan into practical implementation. Activities conducted across JACARDI’s portfolio of over 140 pilots are generating practical implementation evidence on how public health strategies can be translated into practical action to prevent cardiovascular disease and diabetes. The authors argue that coordinated, life course-based approaches, combining prevention, early detection and integrated care, are essential to reduce the burden of these conditions across Europe.
Cardiovascular disease remains the leading cause of premature mortality and disability in the European Union. The article, by lead author Benedetta Armocida and other contributors from the joint action, highlights that the main challenge is not the lack of strategies, but how to implement them effectively and equitably across different health systems.
The article presents JACARDI as a proof-of-concept for implementing the EU Safe Hearts Plan. A key message is that cardiovascular disease and diabetes should be addressed together using a life course approach, recognising that risk factors build up over time. Early actions, such as health literacy programmes for children and young people, can support long-term health outcomes.
Linking detection, care and everyday support
The authors highlight that screening is effective only when it is connected to follow-up care. JACARDI pilots test different approaches, including community-based screening, mobile units and digital tools linked to lifestyle support.
The commentary also emphasises integrated care and self-management. Pilot interventions like a co-designed mobile application to optimize secondary prevention in Madrid and care pathways co-developed with patients and caregivers in the Basque Country demonstrate that digital and telemedicine solutions can support continuity of care and help people manage their condition in everyday life.
Equity and data as key priorities
The article underlines the importance of strong data systems and a focus on equity. Shared data models enable better monitoring of health outcomes and differences between population groups. Inclusive, targeted approaches are needed to ensure that prevention and care reach everyone.
Overall, the commentary highlights that JACARDI provides a practical model for turning policy into action. The authors conclude that combining a life course approach, integrated care and equity-focused implementation can support long-term improvements in cardiovascular health across Europe.
Read more: Commentary on JACARDI and the Safe Hearts Plan
Publication: Closing the implementation gap: the Joint Action on Cardiovascular Diseases and Diabetes (JACARDI) as a proof-of-concept for Europe’s Safe Hearts Plan
Authors: Benedetta Armocida et al. (on behalf of the JACARDI Implementation Board)
Journal: International Journal of Public Health
Publication date: 15 June 2026
DOI: https://doi.org/10.3389/ijph.2026.1609906
INCLIVA brings workplace health education to workers and employers across Spain
INCLIVA, the Health Research Institute of the Hospital Clínico Universitario de València, presented its work within JACARDI at Conecta INCLIVA, a public seminar held on 14 May in Valencia. Bringing together patients, researchers and clinicians, the event offered a space to connect ongoing European research with the people most affected by these conditions and shared the latest scientific advances in cardiovascular health and diabetes.
Cardiovascular diseases remain the leading cause of mortality in Europe, and diabetes already affects one in ten people over the age of 55 in Spain. These figures underline that public engagement with research is not just valuable, but necessary.
The event showcased four active European projects led or supported by INCLIVA‘s cardiovascular research team. The team consists of more than 200 researchers, has produced over 1,300 scientific publications, and currently has nearly 200 active projects and clinical studies. Among these, Dr. Clara Bonanad and Dr. Josep Redón presented JACARDI.
INCLIVA participates in JACARDI as an affiliated entity under FundeSalud, which serves as the Spanish competent authority in the Joint Action. INCLIVA plays an active role across five pilots covering data, screening, prevention, personalised care and health education.
Taking health education into the workplace
Within JACARDI’s health education projects, INCLIVA is developing an online training programme for workers and employers. The initiative aims to equip participants with practical self-care tools, raise awareness about cardiovascular risk, and support the workplace inclusion of people living with these conditions.
The programme consists of ten short five-minute videos, complemented by downloadable materials for all participants. To assess the learning impact, the course includes an evaluation of the knowledge acquired, measures how that knowledge is integrated into daily routines, and solicits participants’ feedback about their experience of the platform. The roll-out of the initiative is currently in progress.
Citizens as partners in research
The event also highlighted citizen science, private philanthropic funding, and the importance of integrating patient perspectives, including a discussion on gender equity in cardiovascular research. One of the event’s special guests, Ms. Maite San Saturnino, President of the Spanish Heart Foundation‘s patient association and an important JACARDI stakeholder, joined in a conversation that opened into a wider audience discussion on the active role citizens can play in scientific progress.
Ms. Mariola Penadés Fons, Director General of Research and Innovation at the Valencian Regional Health Ministry brought the event to a close by highlighting that research only fulfils its purpose when it reaches the people it was always meant to serve. It is precisely this spirit that drives JACARDI’s work and INCLIVA’s commitment to bringing it into workplaces, communities and everyday life.




From a European project to a permanent resource for citizens: how Cantabria is building a sustainable and inclusive health education model
How can a health education initiative continue to generate impact once a European project comes to an end? This is one of the key questions guiding the work carried out in Cantabria by the Nursing Research Group at IDIVAL as part of JACARDI.
The pilot project titled MOOCs to Improve CVD & Diabetes Literacy implemented within JACARDI’s work package on Integrated Care Pathways, aims to improve health literacy and self-care among people living with diabetes and cardiovascular diseases by offering free online courses. Designed for and with patients, the courses help participants better understand their conditions and take an active role in managing their health.
Through this project, the team has developed a free online course aimed at people living with diabetes and cardiovascular disease, designed to improve health literacy and promote self-care. The programme has now reached its fifth edition, engaged more than 150 participants, and more than 90% of those who complete the training consider it highly useful.
By strengthening patients’ knowledge, confidence and self-management skills, the initiative contributes to improving patient pathways in Cantabria, promoting a more informed and active participation in healthcare and supporting long-term disease management.
Building a course with patients, professionals and communities
However, the goal extends beyond the development of a digital educational resource. The project has focused on building a collaborative model involving expert patients, healthcare professionals, researchers, patient associations and the Cantabrian School of Health, with the aim of creating content that is more accessible, relevant and useful for the people it is intended to serve.
“Sustainability is not only about keeping a course active; it is about creating a stable, updatable resource that can continue reaching citizens through different channels,” explains Paula Parás, IDIVAL researcher and coordinator of the pilot programme.
The programme’s continuity is being developed in close collaboration with the Cantabrian School of Health, where the materials created through JACARDI are progressively being integrated into its regular activities to ensure their availability beyond the project’s duration. At the same time, the team is exploring ways for the course to be recommended by physicians and nurses as a complement to routine clinical care.
The courses are freely available online and can be accessed through an online platform.
Equity is another cornerstone of the initiative. To make the training accessible to diverse population groups, IDIVAL collaborates with organisations such as COCEMFE Cantabria, UNATE, Movimiento por la Paz, Fundación Secretariado Gitano, Plataforma Romanés and several adult education centres across the region.
“Chronic diseases require continuous care, and education is essential for helping people better understand their condition and adopt a culture of self-care,” says Mariló Damalia Pineda, Managing Director of COCEMFE Cantabria.
This pilot is closely linked to other JACARDI activities implemented by IDIVAL in Cantabria. Alongside this pilot, the institution is also developing another pilot within JACARDI’s work package on Health Literacy and Awareness, based on online courses for the general population focused on cardiovascular disease prevention, and third pilot as a part of the work package on ‘Patients’ self-management’, aimed at strengthening face-to-face health education workshops through the integration of scientific evidence.
Embedding JACARDI results into Cantabria’s health system
Although these initiatives target different audiences and pursue different objectives, they share a common sustainability strategy through the Cantabrian School of Health, which is part of the Cantabrian Health Service. This collaboration helps ensure that the resources, knowledge and methodologies generated through JACARDI can continue benefiting citizens beyond the lifetime of the project.
This integrated approach has attracted the attention of JACARDI’s European sustainability leaders, who recently visited Cantabria to learn how research, the healthcare system and community organisations are working together to transform project outcomes into long-lasting benefits for citizens.
Workbox for Inclusion: JACARDI helps build workplaces that work for everyone
JACARDI has launched the Workbox for Inclusion, a free, online training programme that helps organisations create more inclusive and health-supportive workplaces. Designed for managers, employers, HR professionals, disability managers and trade union representatives, the Workbox provides practical tools to assess workplace inclusiveness, identify areas for improvement and develop tailored action plans that support employees, including people living with non-communicable diseases such as cardiovascular diseases and diabetes.
Creating working environments that promote health, inclusion and long-term well-being is a key priority for JACARDI. The Workbox for Inclusion contributes to this goal by offering practical support to organisations, with a particular focus on people living with non-communicable diseases (NCDs).
The programme bridges the gap between policy recommendations and everyday practice, especially in small and medium-sized enterprises, by translating public health principles into clear, actionable steps. The Workbox provides tools to assess workplace inclusiveness and to design tailored action plans. These aim to improve employee well-being, support work ability and foster sustainable inclusion.
By combining evidence-based knowledge with practical guidance, the Workbox strengthens organisational capacity and contributes to healthier and more productive workplaces. With initiatives like this, JACARDI continues to take meaningful steps towards a more equitable society, one that enables, supports and empowers all.
The Workbox was developed by the leadership and co-leadership teams responsible for the Work Package on Labour participation of people living with cardiovascular diseases and diabetes within JACARDI. Its design was led by experts from the Istituto Neurologico Carlo Besta (Italy), Poznan University of Medical Sciences, and the Department of Health Prevention (Katedra i Zakład Profilaktyki Zdrowotnej), Poland.
Access the Workbox for Inclusion here.
Download the leaflet here.
Research highlights the potential of self-measurement tools in preventing cardiovascular disease and diabetes
Research conducted within JACARDI summarises evidence on non-clinical methods for measuring blood glucose and cholesterol. The findings point to the preventive potential of self-measurement approaches, while emphasising that wider public health use requires further research, standardisation and strong clinical quality assurance.
Cardiovascular diseases and diabetes are among the leading causes of ill health and premature mortality in Europe. Both conditions are largely preventable, but prevention requires timely data on risk factors and approaches that are accessible to different population groups. Traditional screening methods can be resource‑intensive and may not reach everyone equally.
The researchers reviewed existing evidence on non-clinical measurement methods, such as dried blood spot samples, finger‑prick capillary blood collection, and emerging non‑invasive technologies. Some of these approaches showed close agreement with standard venous blood tests for specific measurements, particularly glycated haemoglobin (HbA1c) and triglycerides.
Clinical standards remain essential
However, the review also makes clear that clinical standards remain essential. Accuracy varies between methods, and differences in sample collection, handling and analysis can affect results. For this reason, self-measurement tools cannot currently replace clinical screening and are not recommended for diagnostic or population-level screening purposes.
“Self-measurement technologies have clear potential to support prevention and reduce barriers to participation,” says researcher (PhD candidate) Hanna Elonheimo, lead author of the study. “At the same time, they should be seen as complementary tools, not alternatives to clinically validated methods.”
The authors highlight that accessible and user‑friendly measurement approaches may still play an important role in increasing awareness of cardiovascular and diabetes risk, supporting disease management, and informing future prevention strategies. Further research is needed to improve standardisation, reliability and regulatory validation before wider implementation can be considered.
Publication: Innovative approaches to early detection of cardiovascular disease and diabetes risk: focus on glucose and cholesterol measuring
Authors: Hanna M Elonheimo, Alexandra Cucu, Gabriela Cristisor, Ciprian Ursu, Claudia Dima, Petru Milos, Giulia Franceschini, Katiuscia Dibiagio, Roberta Papa, Massimiliano Petrelli, Jelka Zaletel, Hanna Tolonen
Journal: European Journal of Public Health
Publication date: 9 February 2026
DOI: https://doi.org/10.1093/eurpub/ckag007
Shaping the EU Safe Hearts Plan: JACARDI joins high-level dialogue on regional and local perspectives
During a high-level discussion bringing together EU and regional stakeholders, JACARDI Coordinator Benedetta Armocida highlighted how coordinated European action can bridge research, policy, and implementation in advancing the EU Safe Hearts Plan. The meeting aimed to explore how regional and local authorities can contribute to shaping and implementing the plan, bringing forward territorial perspectives and feeding into the upcoming Committee of the Regions opinion.
On 6 May 2026, the Interregional Group on Health and Well-being of the European Committee of the Regions, with the support of EUREGHA, hosted the high-level discussion “Shaping the EU Safe Hearts Plan: regional perspectives for cardiovascular health” in Brussels.
The meeting brought together representatives from EU institutions, regional and local authorities, healthcare professionals, researchers, and public health stakeholders to discuss how to advance the implementation of the Safe Hearts Plan (SHP) through stronger multilevel governance and regional action. JACARDI contributed to the discussion as a key European initiative in this field to support the objectives of the SHP.
Cardiovascular diseases remain the leading cause of death and disability in Europe, placing a major burden on individuals, health systems, and economies. Against this backdrop, the discussion highlighted the importance of translating European policy ambitions into concrete and equitable actions adapted to regional and local realities.
Speakers included:
- Carmine Pacente, European Committee of the Regions
- Romana Jerković, European Parliament
- Marianne Takki, European Commission
- Benedetta Armocida, Istituto Superiore di Sanità and Coordinator of JACARDI
- Cristina Gavina, Portuguese Society of Cardiology and European Society of Cardiology
- Antonio Aurigemma, Regione Lazio
The discussion underscored several priorities for the future implementation of the SHP, including strengthening prevention and health promotion, improving early detection and screening, ensuring continuity and integration of care pathways, and addressing persistent inequalities in cardiovascular outcomes, including the cardiovascular gender gap, across and within European regions.
Evidence-informed policies and prevention beyond healthcare settings
Participants also highlighted the growing importance of data systems and digital innovation in supporting evidence-informed and more equitable cardiovascular health policies. At the same time, speakers stressed that effective prevention strategies must extend beyond healthcare settings and reach people directly within schools, workplaces, and local communities, especially underserved populations and people living in vulnerable situations.

Coordinated European action through JACARDI
In this context, Benedetta Armocida presented JACARDI as a concrete example of how coordinated European action can support the objectives of the Safe Hearts Plan by bridging research, policy, and implementation. The Joint Action contributes to strengthening national and regional capacities, fostering collaboration across health systems, and reducing fragmentation in the prevention and management of cardiovascular diseases and diabetes. The discussion concluded with a shared recognition that achieving the ambitions of the EU Safe Hearts Plan will require sustained collaboration between EU, national, regional, and local actors, alongside continued investment in prevention, integrated care, and equity.
The meeting further demonstrated the added value of creating spaces for dialogue between policymakers, researchers, healthcare professionals, and implementers. Bringing together actors operating at different governance levels allows for the exchange of practical experiences, the identification of shared challenges, and the co-development of solutions that are both evidence-based and feasible in real-world settings. Such multistakeholder engagement is essential to ensure that European strategies are translated into sustainable and impactful actions at the regional and local level.
Building stronger prevention systems in Ukraine: insights from the Kyiv JACARDI meeting
A strategic meeting on implementing effective models for the prevention of cardiovascular diseases and type 2 diabetes was held in Kyiv, Ukraine, organized by the Public Health Center of the Ministry of Health of Ukraine within the framework of JACARDI. The event brought together representatives from the Ministry of Health of Ukraine, the WHO Country Office in Ukraine, and regional centers for disease control and prevention. The main goal of the meeting was to strengthen collaboration in public health, exchange experiences, and integrate European best practices into the prevention of non-communicable diseases (NCDs).
Early identification of risk factors, modern community-level screening models, and international experience in prevention programs were at the forefront of discussions, with special attention on the Safe Hearts Plan. Behavioural risk factors and their impact on premature mortality and population health loss were also high on the agenda.
“Non-communicable diseases often remain ‘invisible’ — their consequences do not appear immediately. At the same time, it is important to understand that prevention is far cheaper than treatment, and healthy nutrition and physical activity are not about trends but primarily about preserving health,” said Tetiana Skapa, Director of the Public Health Department of the Ministry of Health of Ukraine.
What JACARDI pilot studies reveal about prevention and care
The meeting also included discussion of the main findings from a study on health literacy regarding self-monitoring of arterial hypertension. The study was conducted using the Ophelia (Optimising Health Literacy and Access) process, a co-design approach for developing health literacy actions that is applied across 24 pilot projects within JACARDI’s work package on health literacy. The findings of the study confirmed that health literacy is a key factor in the effective prevention and self-management of high blood pressure, influencing adherence to treatment and regular monitoring. The study also highlighted practical opportunities for improvement, including clearer patient communication, better access to blood pressure monitoring in community settings, stronger patient education and peer support, and more coordinated healthcare delivery.




Results from another JACARDI pilot project exploring the barriers to prevention and screening for type 2 diabetes were presented. The study found that while primary care is trusted and access to diagnosis and medications is generally good, key barriers persist, including limited access to diagnostics, high administrative burden, short consultation times, and low patient awareness and motivation for prevention, alongside contextual challenges related to war, such as stress and disruption of care. Lifestyle change remains the greatest challenge for patients, and structured education and support programmes are largely absent. Overall, the findings highlight the need to strengthen prevention, improve access to essential diagnostics, and expand patient and professional education.
“Participation in the JACARDI project allows Ukraine to align with European best practices in cardiovascular disease and diabetes prevention and provides a strategic framework that guides our local prevention efforts, supports early detection, and helps us implement evidence-based interventions tailored to the Ukrainian context, particularly in the challenging conditions of war,” said Nataliia Hryb, Specialist in Non-communicable Disease Prevention at the Public Health Center of the Ministry of Health of Ukraine and pilot lead from the Ukrainian team.
Importance of a systemic prevention approach
Participants emphasized the importance of a comprehensive approach to NCD prevention, including improving health literacy and implementing screening programs. The national “Health Screening 40+” program, which provides basic examinations for early detection of cardiovascular diseases, diabetes, and mental health issues, was also discussed.
“Behavioral risk factors remain the key determinants of premature mortality and health loss in Ukraine,” noted Dmytro Shushpanov, Head of the Department of Demographic Modeling and Forecasting at the M. Ptukha Institute for Demography and Social Research, NAS of Ukraine. “At the same time, significant territorial disparities persist, especially in rural areas, which requires strengthening preventive measures and adapting programs to local conditions.”
Next steps and further collaboration
Following the meeting, participants outlined the key directions for future work: strengthening and supporting community-based prevention programs, developing screening initiatives, and increasing public health literacy. The strategic meeting provided an important platform for reinforcing partnerships between state institutions, regional centers for disease control and prevention, and international organizations.
Work ability literacy in action: how Finnish leaders are strengthening workplace resilience
In Finland, the concept of work ability literacy, the knowledge and skills needed to understand, support, and strengthen employees’ capacity to work well, is moving from research into real-world practice. Through JACARDI pilot interventions led by the Finnish Institute of Occupational Health, healthcare and social services leaders are being equipped with tools and strategies that help them support work ability, promote recovery, and lead healthier, more resilient work communities.
The Finnish healthcare system has been undergoing changes for several years. In the reform implemented in 2023, healthcare and social services (HSS) were transferred from municipalities to the responsibility of regional authorities known as wellbeing services counties. This brought significant changes to organizational structures and their operations, as well as to the roles and positions of personnel. The healthcare and social services sector has certain profession-specific work strain factors, such as ethical strain, work pressure and shift work. With the reform, employees had some new stress factors to face: new working methods, in some cases new colleagues and a new organization.
Based on research, work-related stress factors, such as work pressure, job stress, ethical strain, and uncertainty in work, have a significant impact on employees’ well-being. Work stress, shift work and sleep problems related to these increase the risk of cardiovascular diseases (CVD) and type 2 diabetes (T2D). Before the start of JACARDI, in autumn 2023, 38% of Finnish HSS personnel reported lowered work ability and only 35% reported good work recovery. The results are based on the “Mitä kuuluu?” (“How are you?”) study and surveys on well-being at work, conducted for Finnish wellbeing services counties.
Thus, the Finnish Institute of Occupational Health is conducting JACARDI pilots for the Finnish social and healthcare sector aiming to train HSS leaders to better support work ability in their work units. The aim is to increase the work ability literacy of the HSS leaders so that they can support employees who have or are at risk of CVD or T2D, and to support prevention of these diseases. Additionally, the pilots aimed to promote work recovery, health, and work ability through training for so-called work ability partners – employees of the participating work units. These work ability partners are expected to implement tasks that improve work ability in their units alongside their leaders.
What is work ability literacy?
Work ability literacy is defined as the understanding of the demands and the effects of work on one’s health and ability to work, and actions to promote one’s own work ability during work and leisure.
The concept of work ability literacy was developed by the Finnish Institute of Occupational Health. It builds on health literacy principles and the Work Ability House model. It expands health literacy principles to include the context of work, profession, demands and effects of work on work ability, working conditions, and actions to promote and maintain work ability. By promoting work ability literacy, workplaces can better support employees in maintaining health and work capacity, ultimately contributing to improved labor participation for those living with cardiovascular disease and diabetes.
Put on your own oxygen mask first before assisting others
Starting the work at the end of 2023 and at the beginning of 2024, representatives of wellbeing services counties pointed out that the leaders are stressed and overworked, and the first priority should be to enhance their work ability and work recovery. Thus, the training program is initially aimed at helping leaders strengthen their work ability and recovery skills.
The leaders began the training online with four group discussions designed to help them reflect on their situation, identify what is going well and where there is room for improvement, and try out methods to enhance one’s work recovery and work ability. The aim was also to provide opportunities for peer support. Subjects of the training included work recovery, work ability and work ability literacy, lifestyle factors, stress management techniques and psychological flexibility.
Results from the “Mitä kuuluu?” (“How are you?) study and well-being at work surveys conducted for Finnish wellbeing services counties:
Research of the HSS personnel in Finland shows that around 50% of unit supervisors, managers and executive management experience high job demands. However, the management also has high decision latitude, which is why supervisors and managers tend to experience less work stress. 49% to 50% of social and health care unit supervisors, managers and executive management have felt insecurity due to workload exceeding their capacity during the years 2024 and 2025. In autumn 2025, the experiences of uncertainty due to the threat of job termination were most common among managers and executives (32%) as well as unit supervisors (31%).
After the training to improve leaders’ work recovery and work ability, the focus shifts to training aimed at motivating them and teaching them skills to lead work recovery and work ability in their work units, as well as facilitating and supporting the development efforts of their work communities. An important aim is to integrate actions improving work ability into the work processes and structures, such as regular meetings and other recurring events.
The aim is also to support discussions about work ability at the workplace, focusing on work rather than individual work ability. Leaders receive training on how to conduct one-on-one discussions and group discussions. They are also trained on psychological safety within the work community. One of the main tasks in the training is to build an annual cycle for improving work ability.
Simultaneously, with leaders training, there is ongoing partner training for work ability. Work ability partners are employees of the work units, who received training to improve work ability and work recovery in the work units together with the leaders. These partners delivered tasks and challenges for individuals and the community to improve work recovery, health behaviors and mental wellbeing.
The work ability annual cycle as a solution for implementation
The work ability annual cycle compiles key actions that promote work ability and recovery within the workplace community. It helps leaders to systematically lead the development of work ability and recovery. The work ability annual cycle makes the promotion of work ability a shared responsibility, not just for supervisors or management. This applies to both the planning and implementation. The work ability annual cycle integrates the promotion of work ability and recovery into the daily life of the workplace, highlighting small daily actions. Annual planning facilitates operations amidst everyday busyness. It encourages supervisors to reflect on and discuss work ability, and to seek common solutions and development methods with their teams.
Permanent structures for work ability support
During the JACARDI project, the Finnish HSS sector has faced new challenges due to economic difficulties. HSS organizations have been undergoing downsizing. Challenges in HSS in Finland seem to continue, and the need for work ability support is extremely important now and in the future. Permanent structures for work ability support are needed.
Leaders in HSS play a significant role in promoting work ability and work recovery of the work unit. To lead work ability in their units in an ever-changing work environment, they must first take care of themselves. The work ability annual cycle, developed together with the workplace community, can be utilized by embedding the theme of work ability into workplace meetings and thus keeping the theme alive systematically throughout the year.
Learn more at the Finnish Institute of Occupational Health’s dedicated project page.
References
Duchaine, C. S., Aubé, K., Gilbert-Ouimet, M., Vézina, M., Ndjaboué, R., Massamba, V., Talbot, D., Lavigne-Robichaud, M., Trudel, X., Pena-Gralle, A.-P. B., Lesage, A., Moore, L., Milot, A., Laurin, D., & Brisson, C. (2020). Psychosocial Stressors at Work and the Risk of Sickness Absence Due to a Diagnosed Mental Disorder. JAMA Psychiatry, 77(8), Article 8. https://doi.org/10.1001/jamapsychiatry.2020.0322
Gan Y, Yang C, Tong X, Sun H, Cong Y, Yin X, Li L, Cao S, Dong X, Gong Y, Shi O, Deng J, Bi H, Lu Z. Shift work and diabetes mellitus: a meta-analysis of observational studies. Occup Environ Med. 2015 Jan;72(1):72-8. doi: 10.1136/oemed-2014-102150. Epub 2014 Jul 16. PMID: 25030030.
Gao, Y., Gan, T., Jiang, L., Yu, L., Tang, D., Wang, Y., … Ding, G. (2019). Association between shift work and risk of type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of observational studies. Chronobiology International, 37(1), 29–46. https://doi.org/10.1080/07420528.2019.1683570
Hackett RA, Steptoe A. (2017) Type 2 diabetes mellitus and psychological stress – A modifiable risk factor. Nature Reviews Endocrinology, 13(9), Article 9. https://doi.org/10.1038/nrendo.2017.64
Kivimäki M, Kawachi I. (2015) Work Stress as a Risk Factor for Cardiovascular Disease. Current Cardiology Reports, 17(9), 74. https://doi.org/10.1007/s11886-015-0630-8
Laitinen J, Selander K, Ervasti J, ja Kivimäki M. 2024. ”Mitä kuuluu hyvinvointialueiden työhyvinvoinnille 2023”. https://urn.fi/URN:ISBN:978-952-391-148-2. (in Finnish)
Laitinen J, Selander K, Nikunlaakso R, Ervasti J. 2025. ”Mitä kuuluu sosiaali- ja terveydenhuollon työhyvinvoinnille 2024”. https://urn.fi/URN:ISBN:978-952-391-199-4 (in Finnish)
Laitinen J, Nikunlaakso R, Ervasti J, ja Kivimäki M. 2026. ”Mitä kuuluu hyvinvointialueiden työhyvinvoinnille 2025”. https://urn.fi/URN:ISBN:978-952-391-231-1 (in Finnish
Lamiani, G., Borghi, L., & Argentero, P. (2017). When healthcare professionals cannot do the right thing: A systematic review of moral distress and its correlates. Journal of Health Psychology, 22(1), 51–67. https://doi.org/10.1177/1359105315595120
Li W, Chen Z, Ruan W, Yi G, Wang D, Lu Z. (2019) A meta-analysis of cohort studies including dose-response relationship between shift work and the risk of diabetes mellitus. European Journal of Epidemiology, 34(11), 1013–1024. https://doi.org/10.1007/s10654-019-00561-y
Nyberg ST, Fransson EI, Heikkilä K, Ahola K ym. (2014) Job Strain as a Risk Factor for Type 2 Diabetes: A Pooled Analysis of 124,808 Men and Women. Diabetes Care, 37(8), 2268–2275. https://doi.org/10.2337/dc13-2936
Rosa D, Terzoni S, Dellafiore F, Destrebecq A. (2019) Systematic review of shift work and nurses’ health. Occupational Medicine, 69(4), 237–243. https://doi.org/10.1093/occmed/kqz063
Rudkjoebing, L. A., Bungum, A. B., Flachs, E. M., Eller, N. H., Borritz, M., Aust, B., Rugulies, R., Rod, N. H., Biering, K., & Bonde, J. P. (2020). Work-related exposure to violence or threats and risk of mental disorders and symptoms: A systematic review and meta-analysis. Scandinavian Journal of Work, Environment & Health, 46(4), Article 4. https://doi.org/10.5271/sjweh.3877
Salvagioni DAJ, Melanda FN, Mesas AE, González AD, Gabani FL, Andrade SM. de. (2017) Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLOS ONE, 12(10), e0185781. https://doi.org/10.1371/journal.pone.0185781
Sun M, Feng W, Wang F, Li P, Li Z, Li M, Tse G, Vlaanderen J, Vermeulen R, Tse LA. (2018) Meta-analysis on shift work and risks of specific obesity types. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 19(1), 28–40. https://doi.org/10.1111/obr.12621
Xi J, Ma W, Tao Y, Zhang X, Liu L, Wang H. (2025). Association between night shift work and cardiovascular disease: a systematic review and dose-response meta-analysis. Frontiers in Public Health, 2025:13, 1668848. doi: 10.3389/fpubh.2025.1668848
Xie F, Hu K, Fu R, Zhang Y, Xiao K, Tu J. Association between night shift work and the risk of type 2 diabetes mellitus: a cohort-based meta-analysis. BMC Endocr Disord. 2024 Dec 18;24(1):268. doi: 10.1186/s12902-024-01808-w. PMID: 39696306; PMCID: PMC11653577.
Cantabrians take control of their health: new workshops for heart health and diabetes
The Valdecilla Health Research Institute (IDIVAL) is leading and supporting an initiative in Cantabria focused on heart health and diabetes workshops, contributing its expertise in nursing research and community-based interventions to JACARDI.
As an institutional partner of JACARDI, IDIVAL is implementing a pilot scheme within JACARDI’s Work Package 10 focused on patients’ self-management. The pilot aims to support people living with chronic conditions in developing the practical skills and confidence needed to manage their health effectively.
The Nursing Research Group at IDIVAL is supporting the development, communication and implementation of the workshop series called ‘Taking Control of Your Health’ (‘Tomando el control de su salud’). These workshops are an adaptation of an evidence-based intervention created at Stanford University by Kate Lorig. The concept of these workshops is rooted in the Chronic Disease Self-Management Programmes (CDSMP), based on Albert Bandura’s theory of self-efficacy and the Chronic Care Model. The Spanish adaptation ensures that the approach is accessible and relevant to the local context.
Initially implemented in the Cantabria region by the Escuela Cántabra de Salud, it is now responsible for the delivery, development, management of the workshops, and other related initiatives. The local health education center provides logistical support, conducts a multidimensional evaluation of the program, and explores opportunities for further improvement.
Participants learn from each other and strengthen their self-efficacy, as well as their confidence in their ability to act. Seeing peers address similar challenges and achieving small, realistic goals, fosters a strong sense of shared progress. “It helped me to be responsible and not fall into bad health habits, like leading a too sedentary lifestyle”, noted one participant.
Conscious self-care supported
A central element of the sessions is the use of ‘action plans’, which helps participants turn intentions into concrete, achievable commitments.
“In Cantabria, we are observing that when people feel supported and truly heard, change becomes possible”, concludes Gina Lladó, Coordinator of the pilot in Cantabria. “We want these workshops to be more than a standalone initiative. Our aim is for them to become a sustainable tool that can be firmly integrated into the community and reach more and more people over time. What we are seeing during the ongoing implementation encourages us to continue refining and strengthening this initiative”
By equipping people with the skills to manage cardiovascular disease and diabetes, the pilot supports JACARDI’s objectives of promoting health equity, prevention, and sustainable, person-centered care. Ongoing evaluation and collaboration with community partners will inform the program’s future expansion and integration into routine practice.




Diabetes Data Cell: From fragmented data to a national policy tool
Fragmentation of diabetes data poses several challenges across member states. Tackling this issue is a key step towards transforming fragmented diabetes data sets into actionable evidence for smarter health policy. Within JACARDI’s Work Package on Data, the Diabetes Data Cell Project is being developed by Sciensano. The Belgian institute for public health aims to address this question in an effort to optimise patient and healthcare data alignment. The project has recently reached a major milestone: approval by the Belgian Data Protection Authority to link individual-level primary care and specialist clinical datasets with national administrative data on reimbursed healthcare use.
A first data flow covering 2017-2024 has already been completed, resulting in a linked dataset of 76,965 unique individuals living with diabetes across care settings in Belgium. The full governance framework, including legal approvals and secure linkage procedures, has been established and was submitted in December 2025 for publication to BMC Public Health journal. “This marks a crucial step toward building Belgium’s first comprehensive national diabetes dataset,” explain the authors, Astrid Lavens, senior researcher and pilot project coordinator, Kalina Todorova, junior researcher, and Margot Buyle, senior researcher.
What makes this initiative truly unique is how people living with diabetes are identified. Rather than relying on proxy indicators such as therapy use or reimbursement codes, individuals are selected based on the clinical diagnosis recorded in the electronic patient records by their healthcare provider. This ensures a far more accurate and clinically meaningful population definition, a strong foundation for robust real-world evidence.
Primary analyses have already generated valuable insights, such as mapping the overlap between primary and specialist clinical databases and identifying how patients move across levels of care. “For the first time, we can follow individuals across the healthcare system and connect clinical information with data on healthcare utilization and reimbursement,” explain the members of this pilot.
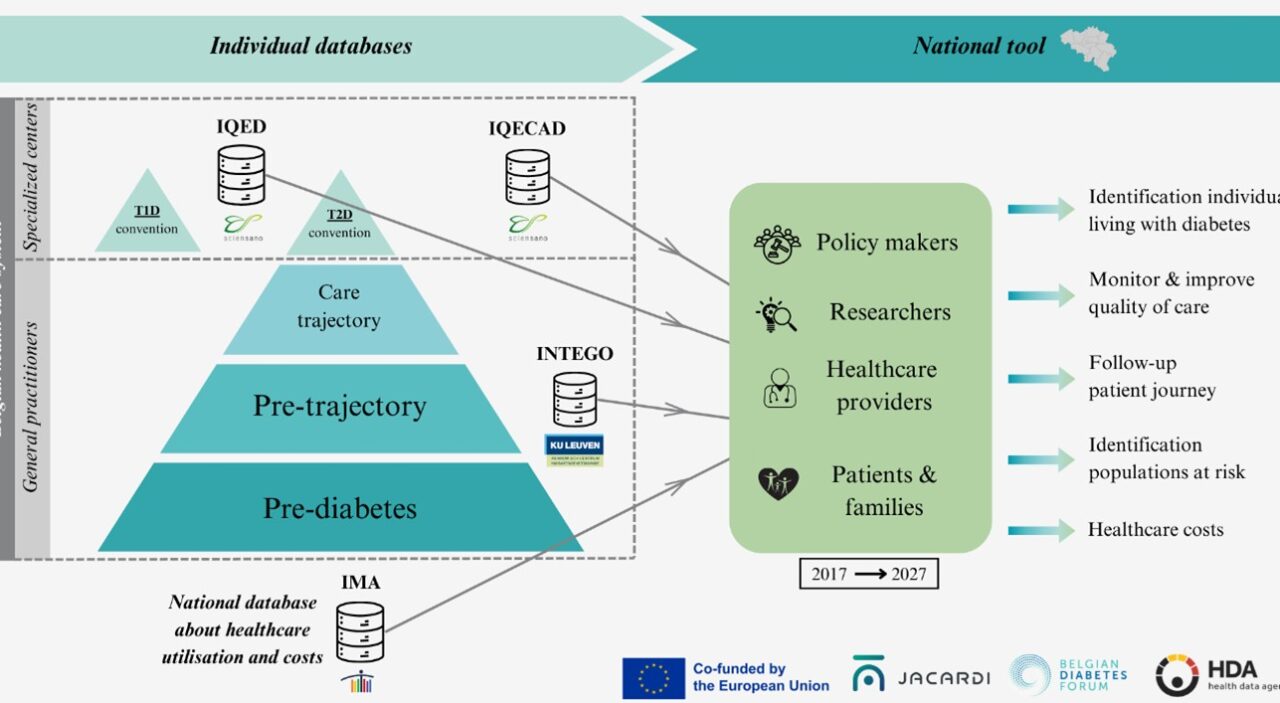
The next phase brings together three institutions: Sciensano, KU Leuven and the Intermutualistic Agency (IMA); each contributing complementary expertise in clinical epidemiology, health services research, and administrative data analysis. By combining these strengths, the consortium – together with the Belgian Diabetes Forum (BEDF) – will transform this linked dataset into a powerful tool for evaluating care quality, treatment patterns, patient pathways, outcomes, and costs.
The Diabetes Data Cell is more than a technical exercise in data linkage. It is a concrete step toward evidence-informed diabetes policy, supporting better planning, improved quality of care, and more efficient resource allocation. By turning routinely collected data into integrated, policy-relevant evidence, this project demonstrates how collaboration within JACARDI can directly strengthen chronic disease monitoring and decision-making at national level, with potential lessons for other countries and other non-communicable diseases.
Strengthening European Health: JACARDI at the JARED Consortium Day
The Joint Action on REspiratory Diseases (JARED) is a major European initiative dedicated to reducing the burden of chronic respiratory diseases through improved prevention, early detection, and integrated care models across the EU. Since chronic conditions like respiratory diseases, diabetes, and cardiovascular issues often share common risk factors, building strategic synergies between Joint Actions is essential to create a unified, high-impact approach to public health and societal prosperity.
In this context, JACARDI contributes to these goals by strengthening prevention and management strategies for cardiovascular diseases and diabetes across Europe within a single framework. By promoting health promotion, reinforcing screening, integrated care pathways and self-management, together with labour participation and improved data governance, JACARDI reinforces a cross-disease, system-based approach that complements JARED’s goals.
Addressing shared risk factors — such as tobacco use, unhealthy diets, physical inactivity, environmental exposures, and social determinants of health — allows both Joint Actions to amplify their impact beyond single disease areas and move toward a more cohesive NCD strategy at EU level.
Building synergies across European public health initiatives
The event program featured a high-level opening with remarks from the WHO and the European Respiratory Society (ERS), followed by a deep dive into JARED’s first-year achievements in indoor air quality, patient pathways, and reaching vulnerable populations. A dedicated session on Strategic Synergies brought together coordinators from various European projects to discuss how to align our efforts for maximum impact.
During this session, Benedetta Armocida, Coordinator of JACARDI presented on building synergies for impact between JACARDI, JARED, and JA PreventNCD, focusing on how coordinated intervention strategies can drive broader societal prosperity. Together, we are ensuring that European health interventions are not just individual projects, but a cohesive movement toward a healthier future.
From pilots to policy: highlights from the Irish JACARDI Heart Health Symposium
The Irish JACARDI Heart Health Symposium took place on 13 February at University College Dublin, bringing together clinicians, researchers, policymakers and programme leads from across Europe. The day showcased the strength of collaboration under JACARDI and the practical progress being made in cardiovascular and diabetes prevention.
The symposium opened with a welcome from Ireland’s Minister for Health, Jennifer Carroll MacNeill, setting the tone of innovation and equity in cardiovascular and diabetes prevention. Dr Benedetta Armocida, Coordinator of JACARDI, provided an overview of JACARDI’s objectives, highlighting the Joint Action’s commitment to shared learning and scalable implementation across Member States.
The spotlight then turned to the pilots – the core of JACARDI. Six pilots from Ireland, Finland, Belgium, Hungary and Ukraine presented their work, with a particular focus on cardiovascular screening and patient self-management.
Pilot presentations: progress across Europe
-
Ireland:
- STOP‑CVD (HSE): Katie Ellwood and Pooja Salgar outlined progress using natriuretic peptide screening to support risk stratification in primary care.
- Healthy Heart Clubs (Croí Heart & Stroke Charity): Lisa Hynes highlighted the importance of structured rehabilitation and long‑term self‑management after cardiac events.
- Finland: Mia Färm (Finnish Diabetes Association) presented the Finnish Risk Calculator, supporting early identification and timely lifestyle intervention.
- Belgium: William Leysen (Diabetes Liga) shared preliminary results from the Halt2Diabetes studies, demonstrating the value of coordinated community‑level screening.
- Hungary: Gréta Máto (OKFŐ) discussed the role of advanced nurse practitioners in strengthening cardiovascular and diabetes screening in primary care.
- Ukraine: Nataliia Hryb (Public Health Centre Ukraine) discussed how they are delivering type 2 diabetes screening in challenging circumstances, underscoring resilience and commitment to patient care.
Across all pilots, a clear message emerged: prevention must be systematic, data-informed and patient-centred.

Women and cardiovascular health: advancing equity
The mid-morning session turned the focus on women with cardiovascular disease (CVD), a key pillar of JACARDI’s commitment to equity and diversity in cardiovascular and diabetes care. The session featured a keynote from JACARDI’s own Dr Héctor Bueno, Co-Leader on the Work Package on Data, who delivered a powerful message: “women are not small men”. His presentation emphasised the need to recognise sex-specific differences in disease presentation, diagnosis, and management.

This was further explored by Dr Mary Ryder, Associate Professor of General Nursing, and Prof. Amy O’Higgins, Consultant Obstetrician at The Coombe Hospital, offering complementary perspectives. Dr Ryder discussed the importance of addressing social determinants of health in cardiovascular prevention, while Prof O’Higgins focused on optimising cardiovascular health during pregnancy, a critical window for long‑term outcomes.
The session was rounded out by a patient story, providing a personal perspective on living with CVD. Her experiences reinforced the human impact behind the statistics and research, leaving a lasting impression on all attendees.
Diabetes and cardiovascular health
The afternoon session turned to diabetes, reflecting its deep interconnection with cardiovascular disease. Dr James (Jim) Januzzi from Harvard Medical School delivered a keynote on heart failure risk across the spectrum of dysglycaemia, stressing the need for integrated approaches. Dr Lisa Devine outlined the successes of Ireland’s Chronic Disease Management Programme, demonstrating how structured, national-level programmes can support early detection, patient engagement, and improved outcomes.
Finally, Prof. Sean Dinneen discussed progress toward a National Diabetes Registry in Ireland, reinforcing the importance of robust data to ensure interventions reach those who need them most, and highlighted the synergies brought about by projects such as JACARDI.
People at the heart of prevention
One of the strongest impressions from the day was how much can be achieved when expertise, curiosity, and compassion are translated into structured action. The symposium wasn’t just about data, tools, or programmes. It was about people: the teams working on the ground across Europe translating strategy into practice, the patients whose stories remind us why these efforts matter, and the exchange of knowledge among colleagues united in a common purpose.
The symposium left attendees not only informed but inspired. It reaffirmed the importance of integrated, patient-centred approaches for a healthier and stronger Europe.