Advancing cardiovascular prevention: regional results from the Italian Health Examination Survey – CUORE Project
Within JACARDI’s framework, the Italian Health Examination Survey (ITA-HES) – CUORE Project has delivered new regional results on major risk factors for non-communicable diseases. Implemented under Work Package 8, the pilot is being carried out in seven Italian regions and is coordinated by the Istituto Superiore di Sanità.
The initiative responds to the World Health Organization recommendation that Member States conduct health examination surveys every five years to monitor progress in prevention and control of non-communicable diseases, particularly cardiovascular diseases.
From data collection to regional action
Screening activities have been completed in four regions – Emilia-Romagna, Piedmont, Liguria and Lazio – and a dedicated report (for 2025) has been distributed to regional stakeholders in each territory.
The survey is based on direct health examinations of random samples of the adult population. It has a dual purpose:
- to strengthen surveillance of cardiovascular and metabolic risk factors through objective measurements;
- to provide population screening for early detection of risk conditions and promote health awareness at individual level.
Regional reports present key indicators recommended for monitoring non-communicable diseases, including:
- Blood pressure: levels, hypertension, awareness and treatment
- Lipid profile: total cholesterol, HDL, triglycerides, hypercholesterolemia, awareness and treatment
- Glycaemic status: blood glucose, diabetes prevalence, awareness and treatment
- Body mass index, obesity, overweight, normal weight, waist and hip circumference
- Nutrition habits based on 24-hour urine collection salt and potassium intake
- Physical activity: inactivity prevalence and daily steps
- Smoking habits: prevalence and cigarette consumption
- Overall absolute cardiovascular risk
Strengthening prevention and equity through evidence
Beyond estimating health indicators, the pilot assessed the impact of screening at individual level, including awareness of risk conditions and opportunities for health promotion. By combining surveillance and prevention, the ITA-HES – CUORE Project supports JACARDI’s objectives to reduce the burden of cardiovascular diseases and diabetes, promote early detection, and improve equity in access to preventive services.
The experience from these four regions demonstrates the feasibility and added value of systematic health examination surveys at regional level. The next steps include completion of activities in the remaining regions and continued collaboration with regional stakeholders to translate findings into targeted prevention policies and actions.
What the results reveal
The analysis of the data collected in the four regions highlights a substantial burden of modifiable cardiovascular risk factors in the adult population, together with important gaps in awareness and treatment. Across regions, elevated blood pressure, high total cholesterol and altered glycaemic status were frequently identified through direct measurements, and a proportion of individuals with these conditions were not aware of their risk status or were not receiving treatment.
In the Piedmont region, 40% of men and 24% of women with hypertension (systolic blood pressure >=140 mmHg and/or diastolic blood pressure >=90 mmHg and/or under specific treatment) were unaware of possible blood pressure problems, and 10% of men and 8% of women who were aware were not receiving treatment.
The results also show relevant levels of overweight and obesity based on body mass index and waist circumference, as well as non-optimal salt intake measured through 24-hour urine collection. In the Emilia-Romagna region, 79% of men and 69% of women were overweight or obese, and more than half of the population consumed more salt than recommended.
In addition, physical inactivity and current smoking remain present in a significant share of the population. Compared to data collected approximately 15 years ago, a common trend in all four regions examined shows a significant reduction in hypercholesterolemia. High cholesterol was defined as having total cholesterol levels of 240 mg/dl or higher, or taking medication to treat it. Overall, the results of main health indicators underline the need for strengthened primary prevention, early detection and targeted health promotion strategies at both national and regional level, in line with JACARDI’s objectives.
Access available results from all regions here.
Cantabrians take control of their health: new workshops for heart health and diabetes
The Valdecilla Health Research Institute (IDIVAL) is leading and supporting an initiative in Cantabria focused on heart health and diabetes workshops, contributing its expertise in nursing research and community-based interventions to JACARDI.
As an institutional partner of JACARDI, IDIVAL is implementing a pilot scheme within JACARDI’s Work Package 10 focused on patients’ self-management. The pilot aims to support people living with chronic conditions in developing the practical skills and confidence needed to manage their health effectively.
The Nursing Research Group at IDIVAL is supporting the development, communication and implementation of the workshop series called ‘Taking Control of Your Health’ (‘Tomando el control de su salud’). These workshops are an adaptation of an evidence-based intervention created at Stanford University by Kate Lorig. The concept of these workshops is rooted in the Chronic Disease Self-Management Programmes (CDSMP), based on Albert Bandura’s theory of self-efficacy and the Chronic Care Model. The Spanish adaptation ensures that the approach is accessible and relevant to the local context.
Initially implemented in the Cantabria region by the Escuela Cántabra de Salud, it is now responsible for the delivery, development, management of the workshops, and other related initiatives. The local health education center provides logistical support, conducts a multidimensional evaluation of the program, and explores opportunities for further improvement.
Participants learn from each other and strengthen their self-efficacy, as well as their confidence in their ability to act. Seeing peers address similar challenges and achieving small, realistic goals, fosters a strong sense of shared progress. “It helped me to be responsible and not fall into bad health habits, like leading a too sedentary lifestyle”, noted one participant.
Conscious self-care supported
A central element of the sessions is the use of ‘action plans’, which helps participants turn intentions into concrete, achievable commitments.
“In Cantabria, we are observing that when people feel supported and truly heard, change becomes possible”, concludes Gina Lladó, Coordinator of the pilot in Cantabria. “We want these workshops to be more than a standalone initiative. Our aim is for them to become a sustainable tool that can be firmly integrated into the community and reach more and more people over time. What we are seeing during the ongoing implementation encourages us to continue refining and strengthening this initiative”
By equipping people with the skills to manage cardiovascular disease and diabetes, the pilot supports JACARDI’s objectives of promoting health equity, prevention, and sustainable, person-centered care. Ongoing evaluation and collaboration with community partners will inform the program’s future expansion and integration into routine practice.




Diabetes Data Cell: From fragmented data to a national policy tool
Fragmentation of diabetes data poses several challenges across member states. Tackling this issue is a key step towards transforming fragmented diabetes data sets into actionable evidence for smarter health policy. Within JACARDI’s Work Package on Data, the Diabetes Data Cell Project is being developed by Sciensano. The Belgian institute for public health aims to address this question in an effort to optimise patient and healthcare data alignment. The project has recently reached a major milestone: approval by the Belgian Data Protection Authority to link individual-level primary care and specialist clinical datasets with national administrative data on reimbursed healthcare use.
A first data flow covering 2017-2024 has already been completed, resulting in a linked dataset of 76,965 unique individuals living with diabetes across care settings in Belgium. The full governance framework, including legal approvals and secure linkage procedures, has been established and was submitted in December 2025 for publication to BMC Public Health journal. “This marks a crucial step toward building Belgium’s first comprehensive national diabetes dataset,” explain the authors, Astrid Lavens, senior researcher and pilot project coordinator, Kalina Todorova, junior researcher, and Margot Buyle, senior researcher.
What makes this initiative truly unique is how people living with diabetes are identified. Rather than relying on proxy indicators such as therapy use or reimbursement codes, individuals are selected based on the clinical diagnosis recorded in the electronic patient records by their healthcare provider. This ensures a far more accurate and clinically meaningful population definition, a strong foundation for robust real-world evidence.
Primary analyses have already generated valuable insights, such as mapping the overlap between primary and specialist clinical databases and identifying how patients move across levels of care. “For the first time, we can follow individuals across the healthcare system and connect clinical information with data on healthcare utilization and reimbursement,” explain the members of this pilot.
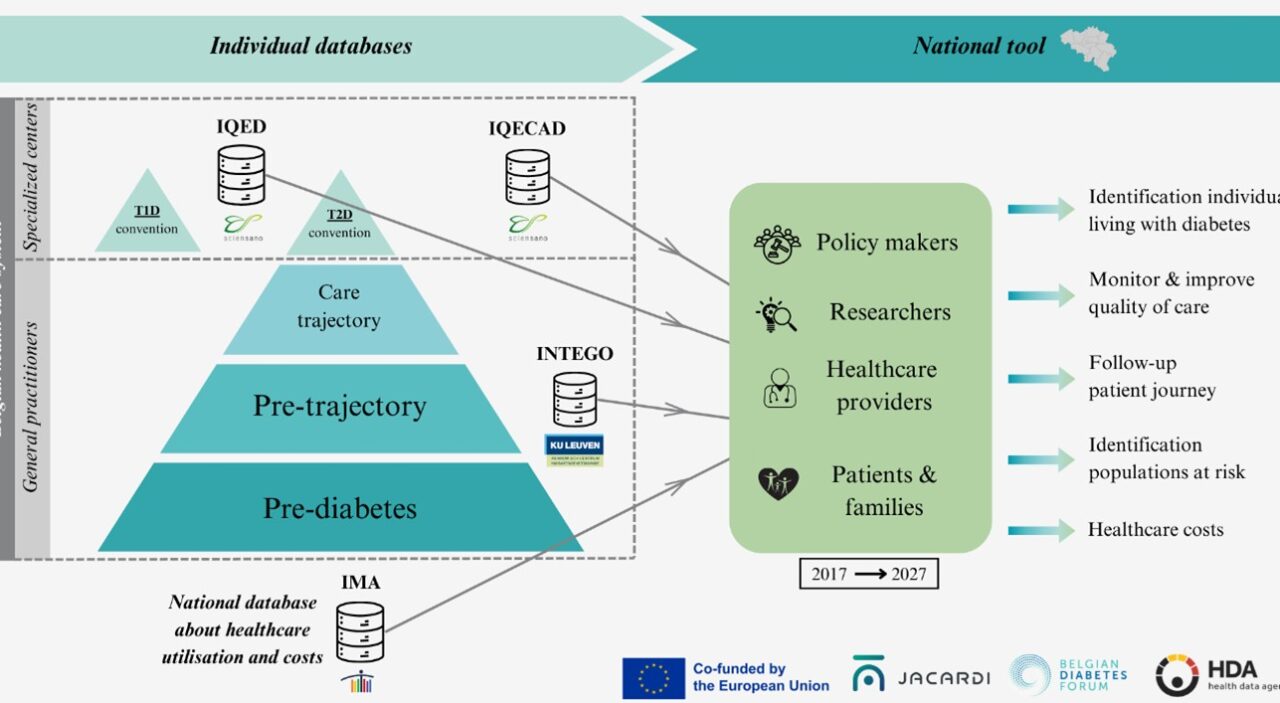
The next phase brings together three institutions: Sciensano, KU Leuven and the Intermutualistic Agency (IMA); each contributing complementary expertise in clinical epidemiology, health services research, and administrative data analysis. By combining these strengths, the consortium – together with the Belgian Diabetes Forum (BEDF) – will transform this linked dataset into a powerful tool for evaluating care quality, treatment patterns, patient pathways, outcomes, and costs.
The Diabetes Data Cell is more than a technical exercise in data linkage. It is a concrete step toward evidence-informed diabetes policy, supporting better planning, improved quality of care, and more efficient resource allocation. By turning routinely collected data into integrated, policy-relevant evidence, this project demonstrates how collaboration within JACARDI can directly strengthen chronic disease monitoring and decision-making at national level, with potential lessons for other countries and other non-communicable diseases.
Three JACARDI pilots showcased at the 45th French Hypertension Days
At the 45th French Hypertension Days in Marseille in December 2025, the French Public Health Agency (Santé publique France) hosted a special session to showcase three innovative JACARDI pilot projects addressing hypertension.
This annual congress, organized by the French Society of Hypertension, brings together more than 500 healthcare professionals from French-speaking countries to share advances in hypertension management.
Session Highlights
The session opened with Dr. Clémence Grave, who presented key French epidemiological insights:
- Hypertension affects over 17 million French adults
- It accounts for nearly 9% of all deaths, yet 1 in 2 adults with hypertension remain unaware of their condition.
To bridge the gap between these alarming statistics and clinical practice, Dr. Grégory Lailler introduced the three main interventions within JACARDI, implemented in the framework of hypertension prevention and health promotion:
- Tension’Elles: A targeted intervention in maternity clinics to raise awareness among women who experienced hypertensive disorders during pregnancy about their future cardiovascular risk, while supporting healthier lifestyle changes. This intervention pilot introduces an innovative care pathway that improves follow-up for women and enhances coordination between hospitals and community care. By identifying risks early, it ensures a seamless transition for women, connecting them with community-health professionals to manage their long-term cardiovascular health and boost the health literacy in these populations.
- TAC (Tension Artérielle – les Chiffres): A public communication campaign to increase awareness of blood pressure numbers and hypertension thresholds, piloted in four high-prevalence French areas.
- TA Tension: A pharmacy-based screening program to identify undiagnosed or uncontrolled hypertension, with loaned self-measurement devices to confirm diagnoses. Leveraging the strategic role of pharmacists as accessible, frontline healthcare providers, this program decentralizes screening. It transforms local pharmacies into key diagnostic hubs, providing patients with low-threshold access to professional medical devices and expert guidance right in their neighborhoods.
Dr. Olivier Obrecht concluded by outlining the National Health Insurance’s nationwide strategies to combat hypertension:
- free self-measurement devices for all newly practicing general practitioners, ensuring better access to diagnostic tools;
- a nationwide awareness campaign to improve hypertension screening rates;
- a newsletter reaching nearly 30 million insured individuals, promoting prevention and early detection;
- an action plan against therapeutic inertia, assessing the effectiveness of antihypertensive treatments after prescription to optimize patient care.
Impact and Outcomes
The session generated strong interest from all healthcare professionals, especially regarding the implementation of new strategies at a national level to tackle the burden of hypertension. It fostered the following:
- Collaboration: a platform for professionals to exchange ideas and refine interventions with national and local stakeholders.
- Network expansion: opportunities to engage with new partners in the JACARDI project and align efforts across France.
The session offered a pivotal moment to unify stakeholders and strengthen collective action against hypertension.
Contributors:
In addition to the main author listed above, this article was prepared with contributions from Santé publique France:
Grégory Lailler, Clémence Grave, Diane Gozlan, Mounia El Yamani, Salima Afiri, Morgane Merat, Andrea Guajardo Villar