Research highlights the potential of self-measurement tools in preventing cardiovascular disease and diabetes
Research conducted within JACARDI summarises evidence on non-clinical methods for measuring blood glucose and cholesterol. The findings point to the preventive potential of self-measurement approaches, while emphasising that wider public health use requires further research, standardisation and strong clinical quality assurance.
Cardiovascular diseases and diabetes are among the leading causes of ill health and premature mortality in Europe. Both conditions are largely preventable, but prevention requires timely data on risk factors and approaches that are accessible to different population groups. Traditional screening methods can be resource‑intensive and may not reach everyone equally.
The researchers reviewed existing evidence on non-clinical measurement methods, such as dried blood spot samples, finger‑prick capillary blood collection, and emerging non‑invasive technologies. Some of these approaches showed close agreement with standard venous blood tests for specific measurements, particularly glycated haemoglobin (HbA1c) and triglycerides.
Clinical standards remain essential
However, the review also makes clear that clinical standards remain essential. Accuracy varies between methods, and differences in sample collection, handling and analysis can affect results. For this reason, self-measurement tools cannot currently replace clinical screening and are not recommended for diagnostic or population-level screening purposes.
“Self-measurement technologies have clear potential to support prevention and reduce barriers to participation,” says researcher (PhD candidate) Hanna Elonheimo, lead author of the study. “At the same time, they should be seen as complementary tools, not alternatives to clinically validated methods.”
The authors highlight that accessible and user‑friendly measurement approaches may still play an important role in increasing awareness of cardiovascular and diabetes risk, supporting disease management, and informing future prevention strategies. Further research is needed to improve standardisation, reliability and regulatory validation before wider implementation can be considered.
Publication: Innovative approaches to early detection of cardiovascular disease and diabetes risk: focus on glucose and cholesterol measuring
Authors: Hanna M Elonheimo, Alexandra Cucu, Gabriela Cristisor, Ciprian Ursu, Claudia Dima, Petru Milos, Giulia Franceschini, Katiuscia Dibiagio, Roberta Papa, Massimiliano Petrelli, Jelka Zaletel, Hanna Tolonen
Journal: European Journal of Public Health
Publication date: 9 February 2026
DOI: https://doi.org/10.1093/eurpub/ckag007
The geography of heart health: Why cardiovascular mortality still depends on where you live in Europe
Cardiovascular disease remains the leading cause of death in the European Union. Yet the risk of dying from it can vary dramatically depending on where people live, reflecting persistent inequalities in prevention, healthcare systems, and public health policies. The Safe Hearts Plan, unveiled by the European Commission on 16 December 2025, as part of an overall health package, offers a chance to close these gaps and advance a shared vision of longer, healthier lives for all Europeans.
What if your country of residence could triple your risk of dying from heart disease?
This reality is one of the key challenges addressed by the EU Safe Hearts Plan, which places a strong focus on geographical inequalities in cardiovascular health across the European Union. The Plan highlights that cardiovascular death rates can be more than six times higher in some Member States than in others, alongside major differences in access to high-quality care and health outcomes.
Across the region, cardiovascular disease (CVD) remains the leading cause of death, yet outcomes vary dramatically between countries. In Bulgaria, for example, the risk of dying from CVD is nearly three times higher than in Denmark, a gap driven not by biology but by differences in prevention, access to care and public health policies. [1]
As Dr Benedetta Armocida, coordinator of JACARDI, explains: “These disparities remind us that cardiovascular health is shaped not only by medical care, but also by the broader social, economic and environmental conditions in which people live.
Addressing them therefore requires a strong and sustained public health approach, one that prioritises prevention, strengthens health systems, and promotes equity in access to effective care and healthier environments. The Safe Hearts Plan offers an important opportunity to reinforce collaboration across countries and sectors, supporting a shared vision for Europe where progress in cardiovascular health benefits all communities and contributes to longer, healthier lives for everyone.”
Progress, but not equally shared
Europe has made significant progress in reducing deaths from CVD over the past decades thanks to advances in treatment and prevention. Yet these gains have not been evenly distributed across the region.
In 2021, CVD still accounted for nearly 28% of deaths in Western Europe, with age-standardised mortality rates of around 107 deaths per 100,000 people. Behind these averages lie stark national differences in risk factors, healthcare systems and prevention policies. [2]
Some countries have demonstrated what is possible when prevention becomes a policy priority. Finland, for example, achieved an 82% reduction in cardiovascular mortality among working-age men between 1972 and 2012 through the North Karelia Project, a pioneering initiative that targeted smoking, cholesterol levels and blood pressure at the community level. The programme demonstrated how sustained prevention policies can dramatically improve cardiovascular health. [3]
Today, similar efforts continue. In Finland, the Finnish Institute for Health and Welfare (THL) is leading a pilot project within JACARDI’s work on screening high-risk populations. The project evaluates how well cardiovascular risk scores predict 10-year CVD risk among migrant populations of Russian, Somali and Kurdish origin, and explores whether recalibrating these tools could improve prevention strategies for diverse populations.
This is just one example among 143 pilot actions implemented across Europe under JACARDI, reflecting a wide geographical diversity and a broad range of health system contexts and target groups. By sharing knowledge and experience across countries, these initiatives help build a stronger evidence base and support the development of more effective and equitable cardiovascular prevention strategies.
Risk factors that still shape Europe’s heart health
Where people live can have a profound impact on their cardiovascular health, a phenomenon often referred to as the “postcode effect”. Beyond individual lifestyle choices or genetic predisposition, factors such as income, education, living conditions, access to healthcare, environmental exposure and local prevention policies all play a crucial role in shaping cardiovascular risk.
Recent evidence highlights how these factors translate into measurable health outcomes. A 2024 study published in JMIR Public Health and Surveillance, analysing 24 Western European countries, found strong associations between cardiovascular mortality and factors such as smoking prevalence and exposure to air pollution. Environmental policies can have a measurable impact: between 2010 and 2019, Europe saw a 19% reduction in heart-disease deaths linked to improvements in air quality. [2]
Despite this progress, many European countries continue to exceed the air pollution thresholds recommended by the World Health Organization. Prevention strategies, including screening programmes and health literacy initiatives, also vary widely between countries. These differences contribute significantly to the persistent cardiovascular health gap across Europe.
The cost of inaction
Beyond the human toll, CVDs impose a significant economic burden, with CVD-related expenditures averaging 630 euros per person in the EU in 2021. As Borjana Pervan, Chief Operating Officer and Deputy CEO of the World Heart Federation, explains:
“In today’s Europe, like elsewhere in the world, where you live still defines your cardiovascular risk. The differences across EU member states are neither genetic nor inevitable but result from gaps in prevention, access to care, and political will. We know what works to close these divides. What’s missing is the sustained commitment to apply it, everywhere, for everyone.”
She adds: “Failure to act comes at a cost: CVD already drains over €280 billion from Europe’s economy every year. With the Safe Hearts Plan now in place, the priority must be to ensure that knowledge is matched by policies and translated into action across all Member States.”
Bridging Europe’s cardiovascular divide
The persistence of these inequalities is one of the key reasons why the European Commission launched the Safe Hearts Plan, aimed at strengthening cardiovascular prevention and care across the EU. Evidence suggests that many disparities in cardiovascular outcomes are avoidable.
According to the JACARDI Context Analysis, differences in cardiovascular health across Europe are closely linked to variations in prevention policies, healthcare system capacity and the implementation of effective cardiovascular health strategies. The analysis also shows that only around half of the EU countries examined have national strategies for cardiovascular screening or health literacy, highlighting the need for stronger and more consistent public health measures.
As the EU moves forward with the Safe Hearts Plan, initiatives like JACARDI play a key role in turning ambition into action. By providing expert guidance, practical experience, and answering to the European Commission’s Call for Evidence, this joint action helps inform initiatives such as the upcoming EU protocol on health checks. Its cross-border collaboration also demonstrates how evidence-based policies and coordinated action can help reduce cardiovascular inequalities and move closer to a shared goal: longer, healthier lives for people across Europe.
With work advancing across all stages of the patient journey, JACARDI is generating valuable evidence across a wide range of contexts and populations. Looking ahead, 2027 will be a key milestone to bring this evidence to 21 countries and help shape national cardiovascular health plans and local policies. By translating and integrating this knowledge across the region, the initiative aims to reduce geographic disparities in prevention, access to care and policy implementation, ensuring that everyone, regardless of where they live, can benefit.
This work aligns with flagship actions under the Plan, such as “EU cares for your heart”, which aim to strengthen national cardiovascular health plans and translate prevention into practice. By sharing and scaling evidence across countries, JACARDI contributes to reducing disparities and improving cardiovascular health outcomes across Europe.
About this series
This article is part of the “Following the Safe Hearts Plan: JACARDI Insights Series”, developed by JACARDI.
The series explores how the EU Safe Hearts Plan, launched by the European Commission on 16 December 2025, is being translated into practice across Europe, highlighting evidence, policy developments and real-world implementation experiences from different health systems.
Through collaboration with a wide range of partners across Europe, including international organisations, patient associations, other European Joint Actions, and global public health bodies, the series aims to unpack how cardiovascular health policies can be translated into concrete action, bridging research, prevention strategies and health system implementation. It also features insights from across the JACARDI community, from the Coordination team and Work Package leaders to pilot voices and implementation experts working directly on the ground.
By combining data, expert perspectives and country-level examples, the series supports a shared understanding of how Europe can reduce cardiovascular inequalities and improve health outcomes for all citizens.
Sources:
[1] Nick Townsend, Melanie Nichols, Peter Scarborough, Mike Rayner, Cardiovascular disease in Europe — epidemiological update 2015, European Heart Journal, Volume 36, Issue 40, 21 October 2015, Pages 2696–2705
[2] Mubarik S, Naeem S, Shen H, Mubarak R, Luo L, Hussain S, Hak E, Yu C, Liu X. Population-Level Distribution, Risk Factors, and Burden of Mortality and Disability-Adjusted Life Years Attributable to Major Noncommunicable Diseases in Western Europe (1990-2021): Ecological Analysis. JMIR Public Health Surveill 2024;10:e57840
[3] Puska P, Jaini P. The North Karelia Project: Prevention of Cardiovascular Disease in Finland Through Population-Based Lifestyle Interventions. Am J Lifestyle Med. 2020 Mar 19;14(5):495-499. doi: 10.1177/1559827620910981. PMID: 32922234; PMCID: PMC7444010.
[4] WHF welcomes the first EU Cardiovascular Health Plan
Shaping the EU Safe Hearts Plan: JACARDI joins high-level dialogue on regional and local perspectives
During a high-level discussion bringing together EU and regional stakeholders, JACARDI Coordinator Benedetta Armocida highlighted how coordinated European action can bridge research, policy, and implementation in advancing the EU Safe Hearts Plan. The meeting aimed to explore how regional and local authorities can contribute to shaping and implementing the plan, bringing forward territorial perspectives and feeding into the upcoming Committee of the Regions opinion.
On 6 May 2026, the Interregional Group on Health and Well-being of the European Committee of the Regions, with the support of EUREGHA, hosted the high-level discussion “Shaping the EU Safe Hearts Plan: regional perspectives for cardiovascular health” in Brussels.
The meeting brought together representatives from EU institutions, regional and local authorities, healthcare professionals, researchers, and public health stakeholders to discuss how to advance the implementation of the Safe Hearts Plan (SHP) through stronger multilevel governance and regional action. JACARDI contributed to the discussion as a key European initiative in this field to support the objectives of the SHP.
Cardiovascular diseases remain the leading cause of death and disability in Europe, placing a major burden on individuals, health systems, and economies. Against this backdrop, the discussion highlighted the importance of translating European policy ambitions into concrete and equitable actions adapted to regional and local realities.
Speakers included:
- Carmine Pacente, European Committee of the Regions
- Romana Jerković, European Parliament
- Marianne Takki, European Commission
- Benedetta Armocida, Istituto Superiore di Sanità and Coordinator of JACARDI
- Cristina Gavina, Portuguese Society of Cardiology and European Society of Cardiology
- Antonio Aurigemma, Regione Lazio
The discussion underscored several priorities for the future implementation of the SHP, including strengthening prevention and health promotion, improving early detection and screening, ensuring continuity and integration of care pathways, and addressing persistent inequalities in cardiovascular outcomes, including the cardiovascular gender gap, across and within European regions.
Evidence-informed policies and prevention beyond healthcare settings
Participants also highlighted the growing importance of data systems and digital innovation in supporting evidence-informed and more equitable cardiovascular health policies. At the same time, speakers stressed that effective prevention strategies must extend beyond healthcare settings and reach people directly within schools, workplaces, and local communities, especially underserved populations and people living in vulnerable situations.

Coordinated European action through JACARDI
In this context, Benedetta Armocida presented JACARDI as a concrete example of how coordinated European action can support the objectives of the Safe Hearts Plan by bridging research, policy, and implementation. The Joint Action contributes to strengthening national and regional capacities, fostering collaboration across health systems, and reducing fragmentation in the prevention and management of cardiovascular diseases and diabetes. The discussion concluded with a shared recognition that achieving the ambitions of the EU Safe Hearts Plan will require sustained collaboration between EU, national, regional, and local actors, alongside continued investment in prevention, integrated care, and equity.
The meeting further demonstrated the added value of creating spaces for dialogue between policymakers, researchers, healthcare professionals, and implementers. Bringing together actors operating at different governance levels allows for the exchange of practical experiences, the identification of shared challenges, and the co-development of solutions that are both evidence-based and feasible in real-world settings. Such multistakeholder engagement is essential to ensure that European strategies are translated into sustainable and impactful actions at the regional and local level.
Building stronger prevention systems in Ukraine: insights from the Kyiv JACARDI meeting
A strategic meeting on implementing effective models for the prevention of cardiovascular diseases and type 2 diabetes was held in Kyiv, Ukraine, organized by the Public Health Center of the Ministry of Health of Ukraine within the framework of JACARDI. The event brought together representatives from the Ministry of Health of Ukraine, the WHO Country Office in Ukraine, and regional centers for disease control and prevention. The main goal of the meeting was to strengthen collaboration in public health, exchange experiences, and integrate European best practices into the prevention of non-communicable diseases (NCDs).
Early identification of risk factors, modern community-level screening models, and international experience in prevention programs were at the forefront of discussions, with special attention on the Safe Hearts Plan. Behavioural risk factors and their impact on premature mortality and population health loss were also high on the agenda.
“Non-communicable diseases often remain ‘invisible’ — their consequences do not appear immediately. At the same time, it is important to understand that prevention is far cheaper than treatment, and healthy nutrition and physical activity are not about trends but primarily about preserving health,” said Tetiana Skapa, Director of the Public Health Department of the Ministry of Health of Ukraine.
What JACARDI pilot studies reveal about prevention and care
The meeting also included discussion of the main findings from a study on health literacy regarding self-monitoring of arterial hypertension. The study was conducted using the Ophelia (Optimising Health Literacy and Access) process, a co-design approach for developing health literacy actions that is applied across 24 pilot projects within JACARDI’s work package on health literacy. The findings of the study confirmed that health literacy is a key factor in the effective prevention and self-management of high blood pressure, influencing adherence to treatment and regular monitoring. The study also highlighted practical opportunities for improvement, including clearer patient communication, better access to blood pressure monitoring in community settings, stronger patient education and peer support, and more coordinated healthcare delivery.




Results from another JACARDI pilot project exploring the barriers to prevention and screening for type 2 diabetes were presented. The study found that while primary care is trusted and access to diagnosis and medications is generally good, key barriers persist, including limited access to diagnostics, high administrative burden, short consultation times, and low patient awareness and motivation for prevention, alongside contextual challenges related to war, such as stress and disruption of care. Lifestyle change remains the greatest challenge for patients, and structured education and support programmes are largely absent. Overall, the findings highlight the need to strengthen prevention, improve access to essential diagnostics, and expand patient and professional education.
“Participation in the JACARDI project allows Ukraine to align with European best practices in cardiovascular disease and diabetes prevention and provides a strategic framework that guides our local prevention efforts, supports early detection, and helps us implement evidence-based interventions tailored to the Ukrainian context, particularly in the challenging conditions of war,” said Nataliia Hryb, Specialist in Non-communicable Disease Prevention at the Public Health Center of the Ministry of Health of Ukraine and pilot lead from the Ukrainian team.
Importance of a systemic prevention approach
Participants emphasized the importance of a comprehensive approach to NCD prevention, including improving health literacy and implementing screening programs. The national “Health Screening 40+” program, which provides basic examinations for early detection of cardiovascular diseases, diabetes, and mental health issues, was also discussed.
“Behavioral risk factors remain the key determinants of premature mortality and health loss in Ukraine,” noted Dmytro Shushpanov, Head of the Department of Demographic Modeling and Forecasting at the M. Ptukha Institute for Demography and Social Research, NAS of Ukraine. “At the same time, significant territorial disparities persist, especially in rural areas, which requires strengthening preventive measures and adapting programs to local conditions.”
Next steps and further collaboration
Following the meeting, participants outlined the key directions for future work: strengthening and supporting community-based prevention programs, developing screening initiatives, and increasing public health literacy. The strategic meeting provided an important platform for reinforcing partnerships between state institutions, regional centers for disease control and prevention, and international organizations.
Equity Lens: Antiracism is integral to reducing health inequalities
Considering the words we use, the decisions we make, and the attitudes we hold, along with recognising discriminatory practices in everyday healthcare settings, are crucial steps public health professionals can take to address health disparities among ethnic minorities. As part of JACARDI’s Equity Lens series, this article examines differences in treatment and care for ethnic minorities, the importance of building trust, and concrete actions professionals can take to achieve more equitable health outcomes.
Since racism directly affects health outcomes, adopting an antiracist approach is integral to quality care, emphasizes Dr. Najma Yusuf, a medical doctor and an antiracism educator for the JACARDI Masterclass titled “Antiracism is care: Advancing Equity in Healthcare”. It is vital to recognize harmful structures, deconstruct them, and avoid past mistakes, especially in the current political climate.
Understanding structural racism and historical context
Racism in healthcare has been well documented and is rooted in structural issues. Studies show that patients from ethnic minorities may receive different treatment than the majority population. This discrepancy is visible even in common medical tests; for instance, in the case of pulse oximetry, which can lead to significant delays in initiating therapy. Diagnosis and treatment decisions made by healthcare professionals can also be influenced by cultural biases.
Dr. Yusuf shed light on the controversial history of medicine, noting that unethical medical experiments conducted on ethnic minorities were a regular occurrence not too long ago. The enduring effects of this history mean that certain minority groups remain wary of healthcare professionals today. Consequently, building trust must begin from the very start, which requires time.
From race-based to race-conscious medicine
A key concern is that race is still used as a risk factor for disease in health research. This persists despite the fact that it has been well-established that race is a social construct, rather than a biological risk factor.
Dr. Yusuf argued that, instead of relying on biology, race should be defined as a social and power construct. This approach allows practitioners to understand and see the effect that race has on an individual’s health and wellbeing. Moving away from race-based medicine toward race-conscious medicine will eventually lead to the reduction of racial health inequalities.
Five concrete ways to promote active antiracism
Antiracism requires active action, and there are concrete ways to promote it within healthcare and healthcare research. Dr. Yusuf presented five actions that professionals can take:
- Admitting the existence of structural racism
- Having active plans to reduce structural racism
- Meeting patients without prejudice
- Disaggregating data in health research for equity monitoring (by country of birth, language, ethnicity)
- Using participatory approaches involving affected communities
Resources:
- Online course on anti-racism for professionals (videos are in Finnish with English subtitles)
- The Moni Suomi Study
- Pulling at the heart: COVID-19, race/ethnicity and ongoing disparities by Chin-Hong, P et al.
- From race-based to race-conscious medicine: how anti-racist uprisings call us to act
- Tackling structural racism and ethnicity-based discrimination in health
About Dr. Najma Yusuf
As a physician specializing in emergency medicine, and an anti-racism expert at the University of Helsinki, Dr. Yusuf has a demonstrated history of working in healthcare, biomedical sciences, and public health. Beyond her medical practice, she is actively engaged in advancing equity and inclusion, serving as a Board Member of the Finnish-Somalia Association (FSA) and as a trainer for doctors in Finland, contributing to a JACARDI pilot program developing antiracist training for healthcare professionals.
About the JACARDI Equity Lens Series:
Throughout this series, we share why equity and diversity are not optional add-ons but core components of truly equitable healthcare as well as a shared responsibility for everyone working in the field. To share the knowledge generated within JACARDI, the Equity Lens article series draws on the JACARDI Equity Masterclass series that provides an in-depth look into matters related to equity and diversity for JACARDI pilot teams conducting 143 healthcare interventions across Europe. The article series offers insights shared by a diverse pool of public health professionals within the consortium. By looking through an equity lens, we can build a more inclusive system for everyone. Join us in learning how an equity lens can shape daily practice and drive meaningful change.
Read the first article in the series: JACARDI’s 4Cs framework for advancing equity and diversity
Advancing cardiovascular prevention: regional results from the Italian Health Examination Survey – CUORE Project
Within JACARDI’s framework, the Italian Health Examination Survey (ITA-HES) – CUORE Project has delivered new regional results on major risk factors for non-communicable diseases. Implemented under Work Package 8, the pilot is being carried out in seven Italian regions and is coordinated by the Istituto Superiore di Sanità.
The initiative responds to the World Health Organization recommendation that Member States conduct health examination surveys every five years to monitor progress in prevention and control of non-communicable diseases, particularly cardiovascular diseases.
From data collection to regional action
Screening activities have been completed in four regions – Emilia-Romagna, Piedmont, Liguria and Lazio – and a dedicated report (for 2025) has been distributed to regional stakeholders in each territory.
The survey is based on direct health examinations of random samples of the adult population. It has a dual purpose:
- to strengthen surveillance of cardiovascular and metabolic risk factors through objective measurements;
- to provide population screening for early detection of risk conditions and promote health awareness at individual level.
Regional reports present key indicators recommended for monitoring non-communicable diseases, including:
- Blood pressure: levels, hypertension, awareness and treatment
- Lipid profile: total cholesterol, HDL, triglycerides, hypercholesterolemia, awareness and treatment
- Glycaemic status: blood glucose, diabetes prevalence, awareness and treatment
- Body mass index, obesity, overweight, normal weight, waist and hip circumference
- Nutrition habits based on 24-hour urine collection salt and potassium intake
- Physical activity: inactivity prevalence and daily steps
- Smoking habits: prevalence and cigarette consumption
- Overall absolute cardiovascular risk
Strengthening prevention and equity through evidence
Beyond estimating health indicators, the pilot assessed the impact of screening at individual level, including awareness of risk conditions and opportunities for health promotion. By combining surveillance and prevention, the ITA-HES – CUORE Project supports JACARDI’s objectives to reduce the burden of cardiovascular diseases and diabetes, promote early detection, and improve equity in access to preventive services.
The experience from these four regions demonstrates the feasibility and added value of systematic health examination surveys at regional level. The next steps include completion of activities in the remaining regions and continued collaboration with regional stakeholders to translate findings into targeted prevention policies and actions.
What the results reveal
The analysis of the data collected in the four regions highlights a substantial burden of modifiable cardiovascular risk factors in the adult population, together with important gaps in awareness and treatment. Across regions, elevated blood pressure, high total cholesterol and altered glycaemic status were frequently identified through direct measurements, and a proportion of individuals with these conditions were not aware of their risk status or were not receiving treatment.
In the Piedmont region, 40% of men and 24% of women with hypertension (systolic blood pressure >=140 mmHg and/or diastolic blood pressure >=90 mmHg and/or under specific treatment) were unaware of possible blood pressure problems, and 10% of men and 8% of women who were aware were not receiving treatment.
The results also show relevant levels of overweight and obesity based on body mass index and waist circumference, as well as non-optimal salt intake measured through 24-hour urine collection. In the Emilia-Romagna region, 79% of men and 69% of women were overweight or obese, and more than half of the population consumed more salt than recommended.
In addition, physical inactivity and current smoking remain present in a significant share of the population. Compared to data collected approximately 15 years ago, a common trend in all four regions examined shows a significant reduction in hypercholesterolemia. High cholesterol was defined as having total cholesterol levels of 240 mg/dl or higher, or taking medication to treat it. Overall, the results of main health indicators underline the need for strengthened primary prevention, early detection and targeted health promotion strategies at both national and regional level, in line with JACARDI’s objectives.
Access available results from all regions here.
Work ability literacy in action: how Finnish leaders are strengthening workplace resilience
In Finland, the concept of work ability literacy, the knowledge and skills needed to understand, support, and strengthen employees’ capacity to work well, is moving from research into real-world practice. Through JACARDI pilot interventions led by the Finnish Institute of Occupational Health, healthcare and social services leaders are being equipped with tools and strategies that help them support work ability, promote recovery, and lead healthier, more resilient work communities.
The Finnish healthcare system has been undergoing changes for several years. In the reform implemented in 2023, healthcare and social services (HSS) were transferred from municipalities to the responsibility of regional authorities known as wellbeing services counties. This brought significant changes to organizational structures and their operations, as well as to the roles and positions of personnel. The healthcare and social services sector has certain profession-specific work strain factors, such as ethical strain, work pressure and shift work. With the reform, employees had some new stress factors to face: new working methods, in some cases new colleagues and a new organization.
Based on research, work-related stress factors, such as work pressure, job stress, ethical strain, and uncertainty in work, have a significant impact on employees’ well-being. Work stress, shift work and sleep problems related to these increase the risk of cardiovascular diseases (CVD) and type 2 diabetes (T2D). Before the start of JACARDI, in autumn 2023, 38% of Finnish HSS personnel reported lowered work ability and only 35% reported good work recovery. The results are based on the “Mitä kuuluu?” (“How are you?”) study and surveys on well-being at work, conducted for Finnish wellbeing services counties.
Thus, the Finnish Institute of Occupational Health is conducting JACARDI pilots for the Finnish social and healthcare sector aiming to train HSS leaders to better support work ability in their work units. The aim is to increase the work ability literacy of the HSS leaders so that they can support employees who have or are at risk of CVD or T2D, and to support prevention of these diseases. Additionally, the pilots aimed to promote work recovery, health, and work ability through training for so-called work ability partners – employees of the participating work units. These work ability partners are expected to implement tasks that improve work ability in their units alongside their leaders.
What is work ability literacy?
Work ability literacy is defined as the understanding of the demands and the effects of work on one’s health and ability to work, and actions to promote one’s own work ability during work and leisure.
The concept of work ability literacy was developed by the Finnish Institute of Occupational Health. It builds on health literacy principles and the Work Ability House model. It expands health literacy principles to include the context of work, profession, demands and effects of work on work ability, working conditions, and actions to promote and maintain work ability. By promoting work ability literacy, workplaces can better support employees in maintaining health and work capacity, ultimately contributing to improved labor participation for those living with cardiovascular disease and diabetes.
Put on your own oxygen mask first before assisting others
Starting the work at the end of 2023 and at the beginning of 2024, representatives of wellbeing services counties pointed out that the leaders are stressed and overworked, and the first priority should be to enhance their work ability and work recovery. Thus, the training program is initially aimed at helping leaders strengthen their work ability and recovery skills.
The leaders began the training online with four group discussions designed to help them reflect on their situation, identify what is going well and where there is room for improvement, and try out methods to enhance one’s work recovery and work ability. The aim was also to provide opportunities for peer support. Subjects of the training included work recovery, work ability and work ability literacy, lifestyle factors, stress management techniques and psychological flexibility.
Results from the “Mitä kuuluu?” (“How are you?) study and well-being at work surveys conducted for Finnish wellbeing services counties:
Research of the HSS personnel in Finland shows that around 50% of unit supervisors, managers and executive management experience high job demands. However, the management also has high decision latitude, which is why supervisors and managers tend to experience less work stress. 49% to 50% of social and health care unit supervisors, managers and executive management have felt insecurity due to workload exceeding their capacity during the years 2024 and 2025. In autumn 2025, the experiences of uncertainty due to the threat of job termination were most common among managers and executives (32%) as well as unit supervisors (31%).
After the training to improve leaders’ work recovery and work ability, the focus shifts to training aimed at motivating them and teaching them skills to lead work recovery and work ability in their work units, as well as facilitating and supporting the development efforts of their work communities. An important aim is to integrate actions improving work ability into the work processes and structures, such as regular meetings and other recurring events.
The aim is also to support discussions about work ability at the workplace, focusing on work rather than individual work ability. Leaders receive training on how to conduct one-on-one discussions and group discussions. They are also trained on psychological safety within the work community. One of the main tasks in the training is to build an annual cycle for improving work ability.
Simultaneously, with leaders training, there is ongoing partner training for work ability. Work ability partners are employees of the work units, who received training to improve work ability and work recovery in the work units together with the leaders. These partners delivered tasks and challenges for individuals and the community to improve work recovery, health behaviors and mental wellbeing.
The work ability annual cycle as a solution for implementation
The work ability annual cycle compiles key actions that promote work ability and recovery within the workplace community. It helps leaders to systematically lead the development of work ability and recovery. The work ability annual cycle makes the promotion of work ability a shared responsibility, not just for supervisors or management. This applies to both the planning and implementation. The work ability annual cycle integrates the promotion of work ability and recovery into the daily life of the workplace, highlighting small daily actions. Annual planning facilitates operations amidst everyday busyness. It encourages supervisors to reflect on and discuss work ability, and to seek common solutions and development methods with their teams.
Permanent structures for work ability support
During the JACARDI project, the Finnish HSS sector has faced new challenges due to economic difficulties. HSS organizations have been undergoing downsizing. Challenges in HSS in Finland seem to continue, and the need for work ability support is extremely important now and in the future. Permanent structures for work ability support are needed.
Leaders in HSS play a significant role in promoting work ability and work recovery of the work unit. To lead work ability in their units in an ever-changing work environment, they must first take care of themselves. The work ability annual cycle, developed together with the workplace community, can be utilized by embedding the theme of work ability into workplace meetings and thus keeping the theme alive systematically throughout the year.
Learn more at the Finnish Institute of Occupational Health’s dedicated project page.
References
Duchaine, C. S., Aubé, K., Gilbert-Ouimet, M., Vézina, M., Ndjaboué, R., Massamba, V., Talbot, D., Lavigne-Robichaud, M., Trudel, X., Pena-Gralle, A.-P. B., Lesage, A., Moore, L., Milot, A., Laurin, D., & Brisson, C. (2020). Psychosocial Stressors at Work and the Risk of Sickness Absence Due to a Diagnosed Mental Disorder. JAMA Psychiatry, 77(8), Article 8. https://doi.org/10.1001/jamapsychiatry.2020.0322
Gan Y, Yang C, Tong X, Sun H, Cong Y, Yin X, Li L, Cao S, Dong X, Gong Y, Shi O, Deng J, Bi H, Lu Z. Shift work and diabetes mellitus: a meta-analysis of observational studies. Occup Environ Med. 2015 Jan;72(1):72-8. doi: 10.1136/oemed-2014-102150. Epub 2014 Jul 16. PMID: 25030030.
Gao, Y., Gan, T., Jiang, L., Yu, L., Tang, D., Wang, Y., … Ding, G. (2019). Association between shift work and risk of type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of observational studies. Chronobiology International, 37(1), 29–46. https://doi.org/10.1080/07420528.2019.1683570
Hackett RA, Steptoe A. (2017) Type 2 diabetes mellitus and psychological stress – A modifiable risk factor. Nature Reviews Endocrinology, 13(9), Article 9. https://doi.org/10.1038/nrendo.2017.64
Kivimäki M, Kawachi I. (2015) Work Stress as a Risk Factor for Cardiovascular Disease. Current Cardiology Reports, 17(9), 74. https://doi.org/10.1007/s11886-015-0630-8
Laitinen J, Selander K, Ervasti J, ja Kivimäki M. 2024. ”Mitä kuuluu hyvinvointialueiden työhyvinvoinnille 2023”. https://urn.fi/URN:ISBN:978-952-391-148-2. (in Finnish)
Laitinen J, Selander K, Nikunlaakso R, Ervasti J. 2025. ”Mitä kuuluu sosiaali- ja terveydenhuollon työhyvinvoinnille 2024”. https://urn.fi/URN:ISBN:978-952-391-199-4 (in Finnish)
Laitinen J, Nikunlaakso R, Ervasti J, ja Kivimäki M. 2026. ”Mitä kuuluu hyvinvointialueiden työhyvinvoinnille 2025”. https://urn.fi/URN:ISBN:978-952-391-231-1 (in Finnish
Lamiani, G., Borghi, L., & Argentero, P. (2017). When healthcare professionals cannot do the right thing: A systematic review of moral distress and its correlates. Journal of Health Psychology, 22(1), 51–67. https://doi.org/10.1177/1359105315595120
Li W, Chen Z, Ruan W, Yi G, Wang D, Lu Z. (2019) A meta-analysis of cohort studies including dose-response relationship between shift work and the risk of diabetes mellitus. European Journal of Epidemiology, 34(11), 1013–1024. https://doi.org/10.1007/s10654-019-00561-y
Nyberg ST, Fransson EI, Heikkilä K, Ahola K ym. (2014) Job Strain as a Risk Factor for Type 2 Diabetes: A Pooled Analysis of 124,808 Men and Women. Diabetes Care, 37(8), 2268–2275. https://doi.org/10.2337/dc13-2936
Rosa D, Terzoni S, Dellafiore F, Destrebecq A. (2019) Systematic review of shift work and nurses’ health. Occupational Medicine, 69(4), 237–243. https://doi.org/10.1093/occmed/kqz063
Rudkjoebing, L. A., Bungum, A. B., Flachs, E. M., Eller, N. H., Borritz, M., Aust, B., Rugulies, R., Rod, N. H., Biering, K., & Bonde, J. P. (2020). Work-related exposure to violence or threats and risk of mental disorders and symptoms: A systematic review and meta-analysis. Scandinavian Journal of Work, Environment & Health, 46(4), Article 4. https://doi.org/10.5271/sjweh.3877
Salvagioni DAJ, Melanda FN, Mesas AE, González AD, Gabani FL, Andrade SM. de. (2017) Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLOS ONE, 12(10), e0185781. https://doi.org/10.1371/journal.pone.0185781
Sun M, Feng W, Wang F, Li P, Li Z, Li M, Tse G, Vlaanderen J, Vermeulen R, Tse LA. (2018) Meta-analysis on shift work and risks of specific obesity types. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 19(1), 28–40. https://doi.org/10.1111/obr.12621
Xi J, Ma W, Tao Y, Zhang X, Liu L, Wang H. (2025). Association between night shift work and cardiovascular disease: a systematic review and dose-response meta-analysis. Frontiers in Public Health, 2025:13, 1668848. doi: 10.3389/fpubh.2025.1668848
Xie F, Hu K, Fu R, Zhang Y, Xiao K, Tu J. Association between night shift work and the risk of type 2 diabetes mellitus: a cohort-based meta-analysis. BMC Endocr Disord. 2024 Dec 18;24(1):268. doi: 10.1186/s12902-024-01808-w. PMID: 39696306; PMCID: PMC11653577.
Equity Lens Series #1: JACARDI’s 4Cs framework brings structure to advancing equity and diversity in diabetes and cardiovascular health
From the outset, JACARDI committed to embedding equity and diversity across all aspects of its work. This ambition includes the design and implementation of our 143 pilot projects across Europe. To share the knowledge generated and make lessons learned widely accessible, JACARDI is launching the Equity Lens article series. Following an introduction to the concept and the tools created, upcoming pieces will draw on the JACARDI Equity Masterclass series, offering insights from a diverse pool of public health professionals within the consortium. Each contribution highlights practical approaches to tackling inequalities in healthcare to improve health outcomes for all.
From the very beginning, the challenge was clear: in order to reduce health inequities, deeply embedded structures reinforcing inequities must be addressed.
How can equity be systematically integrated into practice and policy?
To find answers, we turned to theory, research, consultation with experts, and the extensive collective expertise within our consortium. Based on these, we identified four simple steps that help us move towards equity and inclusion in practice and policy. To make them easy to remember we call them the 4Cs Framework.
The 4Cs Framework
- Critical reflection
- Context and data
- Co-design
- Communication
Together, the 4Cs prompt us to consider what shapes our ways of thinking, who is visible or invisible in the data, who participates in decision-making, and whose voices remain absent. They also encourage us to think intentionally about what we communicate, how we communicate it, and whom it reaches.

Maturity matrix tool and capacity-development activities support continuous learning
To further embed equity in practice, JACARDI developed an equity and diversity maturity matrix that supports JACARDI’s 143 pilot teams all across Europe in planning, implementation, and progress monitoring. In parallel, we introduced a set of capacity-development activities to deepen understanding of practical ways to promote equity and inclusion across diverse contexts.
We are continuing to learn, but early results are highly encouraging. The methods and tools developed within JACARDI are helping teams across Europe integrate equity more systematically. This work has the potential to influence more inclusive and sustainable health policy and practice across Europe.
A detailed description of the methodology, tools, and capacity-building activities can be found in the following publication in BMJ Global Health:
Skogberg N, Spadea T, Armocida B, Zaletel J, Formenti B, Fullaondo A, et al. Embedding equity and diversity principles in a complex multinational setting: methods, tools, capacity development and experiences from the first year of the Joint Action on Cardiovascular Diseases and Diabetes (JACARDI). BMJ Global Health. 2025;10:e019829. https://doi.org/10.1136/bmjgh-2025-019829
Cantabrians take control of their health: new workshops for heart health and diabetes
The Valdecilla Health Research Institute (IDIVAL) is leading and supporting an initiative in Cantabria focused on heart health and diabetes workshops, contributing its expertise in nursing research and community-based interventions to JACARDI.
As an institutional partner of JACARDI, IDIVAL is implementing a pilot scheme within JACARDI’s Work Package 10 focused on patients’ self-management. The pilot aims to support people living with chronic conditions in developing the practical skills and confidence needed to manage their health effectively.
The Nursing Research Group at IDIVAL is supporting the development, communication and implementation of the workshop series called ‘Taking Control of Your Health’ (‘Tomando el control de su salud’). These workshops are an adaptation of an evidence-based intervention created at Stanford University by Kate Lorig. The concept of these workshops is rooted in the Chronic Disease Self-Management Programmes (CDSMP), based on Albert Bandura’s theory of self-efficacy and the Chronic Care Model. The Spanish adaptation ensures that the approach is accessible and relevant to the local context.
Initially implemented in the Cantabria region by the Escuela Cántabra de Salud, it is now responsible for the delivery, development, management of the workshops, and other related initiatives. The local health education center provides logistical support, conducts a multidimensional evaluation of the program, and explores opportunities for further improvement.
Participants learn from each other and strengthen their self-efficacy, as well as their confidence in their ability to act. Seeing peers address similar challenges and achieving small, realistic goals, fosters a strong sense of shared progress. “It helped me to be responsible and not fall into bad health habits, like leading a too sedentary lifestyle”, noted one participant.
Conscious self-care supported
A central element of the sessions is the use of ‘action plans’, which helps participants turn intentions into concrete, achievable commitments.
“In Cantabria, we are observing that when people feel supported and truly heard, change becomes possible”, concludes Gina Lladó, Coordinator of the pilot in Cantabria. “We want these workshops to be more than a standalone initiative. Our aim is for them to become a sustainable tool that can be firmly integrated into the community and reach more and more people over time. What we are seeing during the ongoing implementation encourages us to continue refining and strengthening this initiative”
By equipping people with the skills to manage cardiovascular disease and diabetes, the pilot supports JACARDI’s objectives of promoting health equity, prevention, and sustainable, person-centered care. Ongoing evaluation and collaboration with community partners will inform the program’s future expansion and integration into routine practice.




Diabetes Data Cell: From fragmented data to a national policy tool
Fragmentation of diabetes data poses several challenges across member states. Tackling this issue is a key step towards transforming fragmented diabetes data sets into actionable evidence for smarter health policy. Within JACARDI’s Work Package on Data, the Diabetes Data Cell Project is being developed by Sciensano. The Belgian institute for public health aims to address this question in an effort to optimise patient and healthcare data alignment. The project has recently reached a major milestone: approval by the Belgian Data Protection Authority to link individual-level primary care and specialist clinical datasets with national administrative data on reimbursed healthcare use.
A first data flow covering 2017-2024 has already been completed, resulting in a linked dataset of 76,965 unique individuals living with diabetes across care settings in Belgium. The full governance framework, including legal approvals and secure linkage procedures, has been established and was submitted in December 2025 for publication to BMC Public Health journal. “This marks a crucial step toward building Belgium’s first comprehensive national diabetes dataset,” explain the authors, Astrid Lavens, senior researcher and pilot project coordinator, Kalina Todorova, junior researcher, and Margot Buyle, senior researcher.
What makes this initiative truly unique is how people living with diabetes are identified. Rather than relying on proxy indicators such as therapy use or reimbursement codes, individuals are selected based on the clinical diagnosis recorded in the electronic patient records by their healthcare provider. This ensures a far more accurate and clinically meaningful population definition, a strong foundation for robust real-world evidence.
Primary analyses have already generated valuable insights, such as mapping the overlap between primary and specialist clinical databases and identifying how patients move across levels of care. “For the first time, we can follow individuals across the healthcare system and connect clinical information with data on healthcare utilization and reimbursement,” explain the members of this pilot.
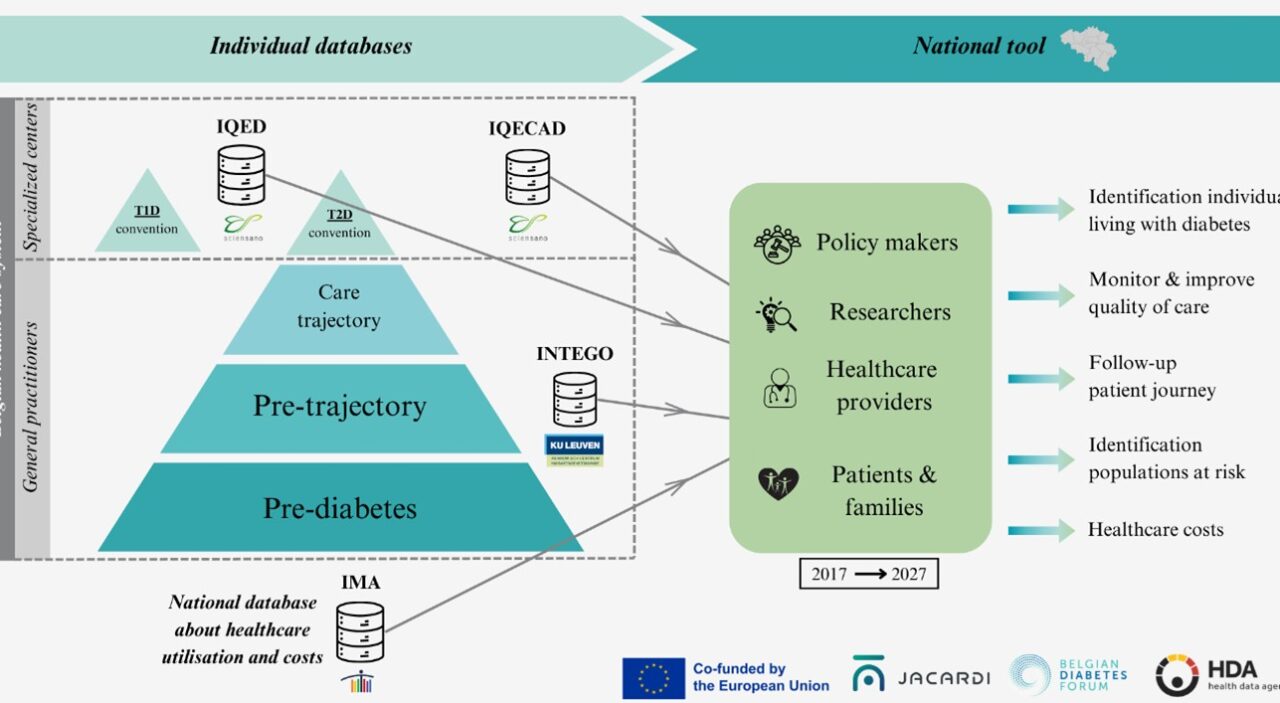
The next phase brings together three institutions: Sciensano, KU Leuven and the Intermutualistic Agency (IMA); each contributing complementary expertise in clinical epidemiology, health services research, and administrative data analysis. By combining these strengths, the consortium – together with the Belgian Diabetes Forum (BEDF) – will transform this linked dataset into a powerful tool for evaluating care quality, treatment patterns, patient pathways, outcomes, and costs.
The Diabetes Data Cell is more than a technical exercise in data linkage. It is a concrete step toward evidence-informed diabetes policy, supporting better planning, improved quality of care, and more efficient resource allocation. By turning routinely collected data into integrated, policy-relevant evidence, this project demonstrates how collaboration within JACARDI can directly strengthen chronic disease monitoring and decision-making at national level, with potential lessons for other countries and other non-communicable diseases.
Diabetes education course supports the Bangladeshi community in the Marche region
In November 2024, the Marche region concluded the first edition of a free Type 2 diabetes education course in Ancona, in collaboration with the ANOLF Association (Associazione Nazionale Oltre le Frontiere), and organised within the European joint action JACARDI by the Marche region, the regional health agency of the Marche region and the Marche diabetes network. The initiative aimed to improve access to prevention, information and healthcare services for the Bangladeshi community by overcoming linguistic and cultural barriers through culturally adapted education, developed through the collaboration established with the ANOLF Association.
Participants shared how valuable the course was for their daily lives. Roxina Akther, a course participant, said the training helped her better understand how to manage diabetes through doctors’ advice, healthy diet and daily habits, and encouraged her to share this knowledge with friends and the wider community. Romana Abdur, a Bangladeshi cultural mediator working with ANOLF, highlighted how culturally adapted guidance supports community members who do not speak Italian in accessing information and healthcare services with greater confidence.
Watch the video to hear and see the community’s perspective.

Breastfeeding and the first 1000 days: an overlooked frontier for disease prevention and health promotion in Europe
Guest article by :
Angela Giusti, Francesca Zambri, Vincenza Di Stefano, Annachiara Di Nolfi, Flavia Splendore (Italian National Institute of Health, Italy), Anne Bærug, Ann-Magrit Lona, Hanne Christine Mosand Bliksås, Gry Hay (Norwegian Directorate of Health, Norway)
JACARDI is proud to feature this guest article from the JA PreventNCD team on Baby Friendly Communities and Health Services. The piece shows how breastfeeding and the first 1000 days are a crucial, yet often overlooked, opportunity to prevent noncommunicable diseases in Europe.
JACARDI represents one of the most ambitious and comprehensive efforts Europe has undertaken to reduce the burden of cardiovascular disease (CVD) and type 2 diabetes. Its life-course approach, its commitment to equity, and its attention to the social and commercial determinants of health create a uniquely fertile ground for expanding the reach of prevention upstream. In this special guest article, the JA PreventNCD team shares their perspective on one such upstream dimension: the first 1000 days of life, from pregnancy to a child’s second birthday. The evidence linking breastfeeding to reduced long-term risk of CVD and type 2 diabetes, in both children and mothers, is now robust, consistent, and biologically grounded.
A Consistent Body of Evidence
Over three decades of research have produced a compelling and converging picture: protecting, promoting, and supporting breastfeeding are among the most effective interventions available for reducing the lifetime risk of the two conditions at the heart of JACARDI’s mandate. The effect sizes are clinically meaningful, dose-related, and supported by plausible biological mechanisms making a strong public health case for action.
Dr. Nigel Rollins, professor at Queen’s University Belfast and one of the lead authors of the Lancet Breastfeeding Series, recently participated in a webinar organized by JA PreventNCD, presenting data on the lifelong effects of human milk. As that landmark series established, and as subsequent systematic reviews have consistently confirmed, having been breastfed as a child is associated with a 26% reduction in the probability of childhood overweight and obesity, falling to a still significant 13% when restricted to high-quality studies adjusting for confounders. Obesity, in turn, is one of the strongest modifiable risk factors for both diabetes and cardiovascular disease.
The Maternal Dimension: Prevention Starts at the Source
The protective effects of breastfeeding are not confined to the child. Mothers who breastfeed also accumulate significant cardiometabolic protection and given that CVD is the leading cause of death in women across Europe, this dimension deserves greater prominence in prevention policy.
A systematic review and meta-analysis drawing on data from over 1,19 million parous women (i.e., women who have given birth) across 8 studies, found that women who had ever breastfed had an 11% reduction in all-cause cardiovascular disease, a 14% reduction in coronary heart disease, a 12% reduction in stroke, and, most strikingly, a 17% reduction in fatal cardiovascular events. A complementary prospective study of nearly 300 000 women replicated these findings across a different population context, confirming a dose-related effect: longer breastfeeding duration consistently lowered risk.
For diabetes specifically, a systematic review found breastfeeding associated with a 27% lower risk of type 2 diabetes in mothers, rising to a 34% risk reduction among women with a history of gestational diabetes, precisely the group at highest risk of progression to overt type 2 disease. A 2025 meta-analysis confirmed a 36% reduced risk of type 2 diabetes mellitus in women with gestational diabetes who breastfed, while non-exclusive breastfeeding in this group was associated with a 76% increased risk, a stark illustration of what suboptimal support costs.
Beyond statistics: biological plausibility
A legitimate scientific question is whether an intervention as simple and as early as infant feeding could plausibly exert effects on cardiometabolic health decades later. The evolving science of human milk composition provides a compelling answer. Breastmilk is not a fixed nutritional formula: it contains maternal gut bacteria, immune cells primed in the mother’s intestine, human milk oligosaccharides that actively shape the infant’s microbiome, small RNAs that regulate gene expression in the baby, and exosomes that carry epigenetic signals. It is, as researchers in the field put it, a complex biological dyadic system, much more than a combination of synthetic ingredients.
The infant gut microbiome established in the first year of life differs markedly between breastfed and formula-fed babies, and these differences persist into childhood and beyond, with downstream effects on immune regulation, metabolic programming, and inflammatory tone. These are precisely the mechanisms through which early-life exposures translate into adult disease trajectories. Breastfeeding does not merely nourish; it calibrates systems.
Enabling informed choice
Understanding the biological depth of breastfeeding does not translate into an obligation. Women, families, have the right to make informed decisions about how they feed their babies, and that right is only meaningful when it rests on genuine access to accurate information, skilled support, and environments that make healthy choices feasible. As the WHO European Strategy for the Prevention and Control of Noncommunicable Diseases “Gaining Health” established nearly two decades ago, the goal of public health is not to tell people what to do, but to make the healthy choice the easy choice. This principle applies with particular force in the first 1000 days, a period in which families are navigating major biological, psychological, and social transitions, often with limited support.
The evidence reviewed here and presented at the JA PreventNCD webinar underscores why that support matters at a systemic level. Breastfeeding rates across Europe remain well below WHO recommendations, and the barriers are rarely individual: they include inadequate parental leave policies, lack of workplace accommodation, aggressive commercial marketing of breastmilk substitutes, and insufficient access to skilled lactation support. These are structural determinants, not personal failures. Collective responsibility, of health systems, employers, policymakers, and communities, means addressing those structures, so that women and families who wish to breastfeed are genuinely able to do so, and those who cannot or choose not to are supported without stigma or judgment.
European Joint Actions and the first 1000 days: a shared foundation
The evidence presented here is not only of academic relevance, it is already informing coordinated action across Europe. Within JA PreventNCD, the Joint Action on Prevention of Non-Communicable Diseases and Cancer, Work Package 6 is dedicated to promoting healthy living environments, and Task 6.5 focuses on implementing the Baby-Friendly Community and Health Services (BFCHS), evaluated as a Best Practice for NCD prevention by the EU Commission in 2022.
Coordinated by the Italian National Institute of Health in partnership with the Norwegian Directorate of Health, this task is implementing the BFCHS model across seven European countries (Greece, Italy, Lithuania, Norway, Slovenia, Spain, and Ukraine) with a specific aim of increasing breastfeeding rates as a contribution to reducing NCDs incidence, starting from the first 1000 days of life, with a focus on social and health inequalities.
The convergence between JA PreventNCD and JACARDI’s mandate is both natural and consequential. Both actions are grounded in a life-course and equity-oriented approach, addressing the social and commercial determinants that shape health trajectories. The science of the first 1000 days, and of breastfeeding, offers a shared evidence base that connects upstream prevention with the downstream outcomes that JACARDI is working to reduce. What begins in the first weeks of life can still be measured, in cardiovascular risk registers and diabetes incidence data, decades later.
Future European Joint Actions and NCD strategies may find in the first 1000 days not a parallel track, but an integral part of the life-course continuum that prevention policy is already committed to addressing.