New RESIL-Card tool supports resilient and equitable cardiovascular care across Europe
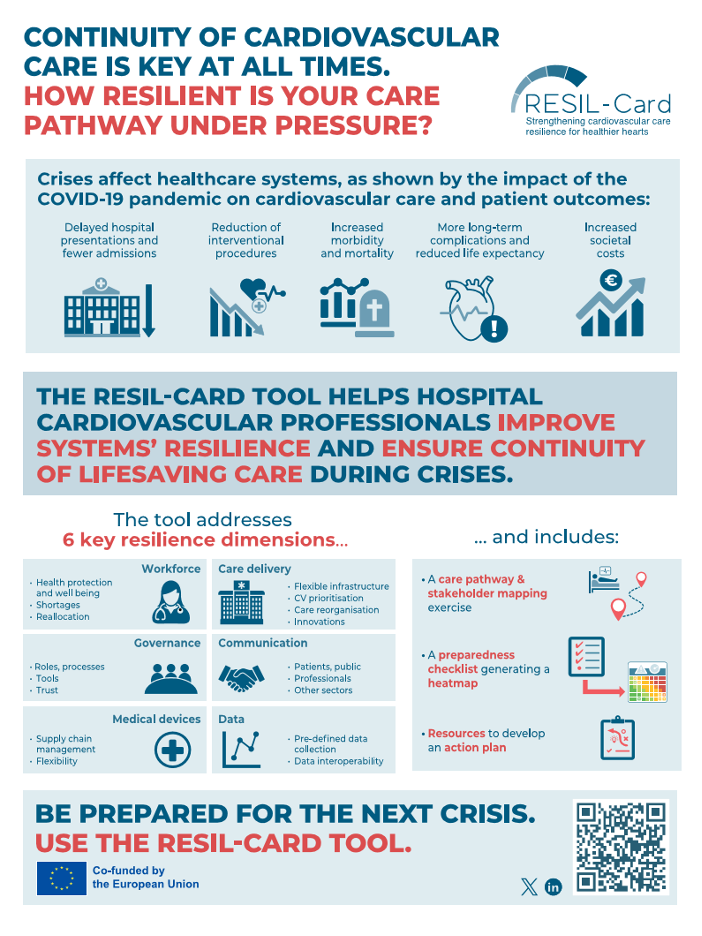
A new online tool called RESIL-Card has been recently launched to help European healthcare professionals strengthen the resilience of cardiovascular care pathways and safeguard the continuity of lifesaving care during times of crisis.
The free resource was developed through the eponymous project, which is co-funded under the EU4Health Work Programme and led by the We CARE advocacy group. It provides a structured framework for assessing preparedness and identifying practical actions to ensure that essential cardiovascular services remain accessible when health systems are facing disruption.
Cardiovascular diseases remain the leading cause of death in Europe, making uninterrupted access to diagnosis, treatment and follow-up care a major public health priority. Following the COVID-19 pandemic and recent challenges, vulnerabilities in healthcare systems have been exposed, emphasising the importance of stronger preparedness planning. RESIL-Card was developed to help healthcare organisations move beyond crisis response and build resilience into routine service delivery.
Strengthening preparedness through collaboration and evidence
RESIL-Card is designed “by and for” hospital multidisciplinary teams involved in cardiovascular care. Through a structured, four-step self-assessment process, users can evaluate the preparedness of their care pathways, identify strengths and gaps, and define tailored actions to support and leverage improvement.
The tool was developed through an extensive co-creation process involving clinicians, public health experts, patient representatives, and policymakers from across Europe. By combining scientific evidence, existing preparedness frameworks and real-world experience, RESIL-Card translates resilience concepts into practical actions that can be implemented in diverse healthcare settings and geographies.
“The value of the RESIL-Card tool is that it gives our team a structured way to identify gaps we had intuitively recognised but never formally addressed,” says an early adopter of the tool.
Supporting JACARDI’s vision for stronger health systems
RESIL-Card’s objectives closely support JACARDI’s efforts to strengthen prevention, care pathways and health system sustainability across Europe. By helping healthcare organisations assess vulnerabilities, improve preparedness, and maintain the continuity of cardiovascular services during periods of disruption, the tool contributes to creating more sustainable and equitable health systems for people living with cardiovascular disease.
The initiative is also aligned with key European policy priorities, notably the EU Safe Hearts Plan and the health preparedness pillar of the EU Preparedness Union Strategy. RESIL-Card’s practical assessment framework helps translate these strategic objectives into concrete actions that healthcare providers can implement to strengthen preparedness, protect access to care and improve long-term system resilience.
By helping healthcare teams anticipate risks, improve coordination and strengthen service continuity, the tool supports a proactive approach to quality improvement and preparedness. It also encourages a patient-centred approach by prompting healthcare providers to identify and address vulnerabilities that could impact access to diagnosis, treatment and follow-up care. In doing so, RESIL-Card can help reduce inequalities in access to cardiovascular services and improve outcomes for people living with cardiovascular disease, particularly during periods of disruption.
“Cardiovascular care must remain uninterrupted regardless of the challenges health systems face. The RESIL-Card tool provides healthcare teams with a practical way to assess preparedness, identify improvement opportunities, and ultimately ensure that patients continue to receive lifesaving care when it matters most,” says Professor William Wijns, Research Professor in Interventional Cardiology at the University of Galway (Ireland) and coordinator of the RESIL-Card initiative.
By providing a common framework for assessing and strengthening preparedness, RESIL-Card contributes to ongoing European efforts to build more resilient health systems, promote the exchange of good practices across Member States, and support the implementation of strategies aimed at improving cardiovascular health, reducing inequalities and ensuring continuity of care during future crises.
RESIL-Card is already gaining traction across Europe, supported by national interventional cardiology working groups and hospitals that are helping drive its dissemination and implementation.
The tool is freely available through multiple dissemination channels to healthcare professionals, healthcare organisations, hospital groups, policymakers and other stakeholders who are committed to strengthening cardiovascular care resilience and protecting access to high-quality care for all, especially when it is needed most.
Read more
Access the online RESIL-Card tool here
Learn more about the RESIL-Card initiative
{kind=link}
Relearning life after a heart attack: How patients are shaping their recovery
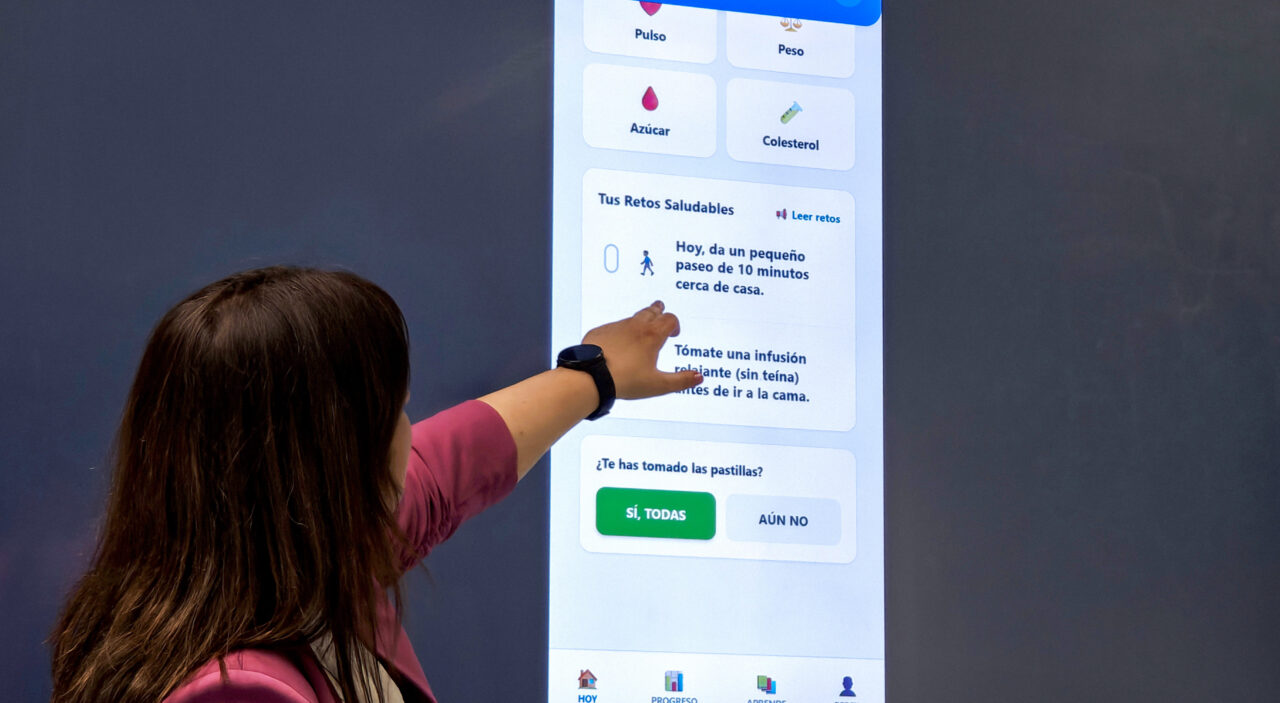
Through JACARDI´s AMIGA (Acute Myocardial Infarction Guidance and Adherence) pilot project, patients, clinicians, and researchers at Hospital 12 de Octubre in Madrid (Spain) and the Spanish National Centre for Cardiovascular Research (CNIC) are co-creating a mobile app to support life after a heart attack, turning uncertainty into guidance, and recovery into a shared journey.
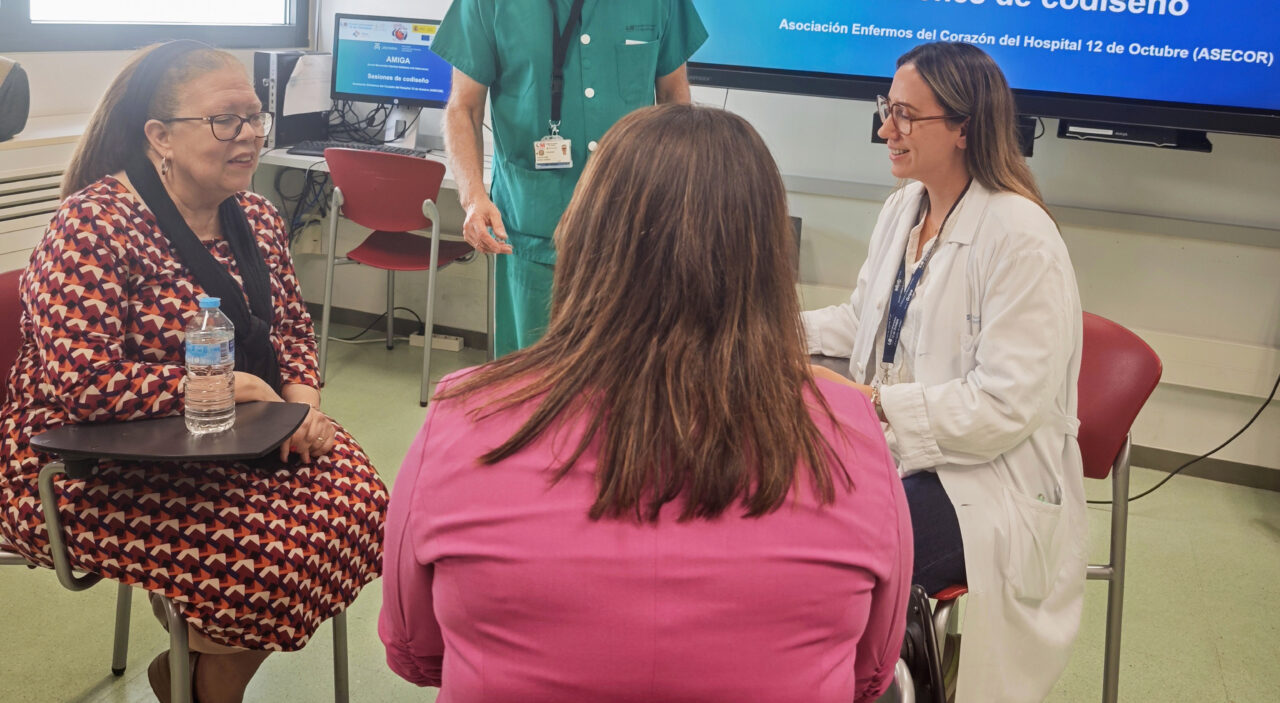
When María Eugenia left the hospital after her heart attack, she didn’t just carry a discharge report, she carried uncertainty. “This session felt timely and necessary for patients who leave the hospital feeling a bit lost or overwhelmed”, she says, speaking about one of the recent co-design sessions organised within the AMIGA pilot project at Hospital 12 de Octubre in Madrid (Spain).
AMIGA is part of JACARDI’s Work Package on patients’ self-management. Led by Hospital 12 de Octubre and the Spanish National Centre for Cardiovascular Research (CNIC), it focuses on improving self-management after a heart attack through a co-designed mobile application.
María Eugenia’s words capture a moment that many patients will recognize: the transition from hospital to home, when clinical care gives way to self-care and questions often outnumber answers. It is precisely in this vulnerable period where the project aims to make a difference.
The initiative is led by Dr Héctor Bueno, cardiologist and scientific director of the Cardiovascular Research Area at the i+12 Research Institute, Hospital Universitario 12 de Octubre, in Madrid; leader of the JACARDI working group on data availability and quality; and leader of a research group at CNIC.
A digital companion for life after a heart attack
The AMIGA pilot is developing a mobile application designed to support people recovering from a heart attack. Grounded in principles of positive psychology, the app aims to enhance therapeutic adherence and empower patients in their day-to-day self-care.
Fifteen participants, most aged between 70 and 75, took part in individual sessions simulating the real patient journey: from recruitment into the program to hands-on interaction with the app. Among them, one participant stood out as a powerful reflection of the project’s ambition: a 95-year-old woman who became one of its key advisors.
Behind this pilot lies a broader vision. Managing cardiovascular disease and diabetes depends not only on what happens inside hospitals, but largely on what patients are enabled to do in their everyday lives.
JACARDI’s Work Package on patients’ self-management focuses precisely on strengthening that capacity. Its pilot projects explore how patients can be better supported to adopt healthier lifestyles, monitor their symptoms, follow treatments correctly, and communicate more effectively with healthcare professionals, especially nurses, who play a vital role in this project. Equally important, they address something less visible but not less critical: how people cope with the emotional and practical challenges of living with a chronic condition.
When patients are equipped and confident to manage their health, outcomes improve, not only in terms of quality of life, but also through reduced avoidable complications and lower pressure on health systems.
Listening before building
These sessions were not only about testing technology; they were about understanding people, how they think, what they need and where they struggle. As Dr Bueno explains, this approach is not just desirable, it is essential:
“Many digital health solutions are developed without direct patient involvement, often resulting in low usage and adherence rates. In addition, given that the typical profile of these patients tends to be older, designing a digital tool that is accessible to individuals with potentially low digital literacy presents an additional challenge,” explains Dr Bueno.
The AMIGA project places patients at the centre of the design process, shaping everything from language and tone to usability and content.
Building together
The sessions were enriched by the involvement of ASECOR, the Association of Cardiac Patients at Hospital 12 de Octubre, bringing lived experience and a strong sense of community into the process.
As Antonio Sánchez, President of ASECOR, highlights, “it’s important not only to give visibility to these diseases, but also to raise awareness through the experiences of the patients participating in the project.” That perspective is grounded in long-standing collaboration with the hospital, which Carlos Quijorna, Treasurer of ASECOR, describes as “contributing our grain of sand.”
Ultimately, the value of the initiative lies in something deeply human: reducing the sense of isolation many patients feel after discharge. As Luis Álvarez, Secretary of ASECOR, puts it, “this application helps patients who, until now, often felt alone. With this, they feel more supported and can consult about their own condition.”
Co-design as a path to impact
These sessions are part of an ongoing process involving patients, caregivers, healthcare professionals, researchers, and technology experts. Each conversation, each piece of feedback, helps transform the app into something more than a digital tool, it becomes a reflection of real needs, real concerns, and real lives.
For the JACARDI pilot, this approach maximizes the likelihood of real-world impact. For participants, it offers something equally valuable: the chance to shape a solution that could improve the lives of future patients.
And for people like María Eugenia, it turns a moment of uncertainty into one of purpose.


Research highlights the potential of self-measurement tools in preventing cardiovascular disease and diabetes
Research conducted within JACARDI summarises evidence on non-clinical methods for measuring blood glucose and cholesterol. The findings point to the preventive potential of self-measurement approaches, while emphasising that wider public health use requires further research, standardisation and strong clinical quality assurance.
Cardiovascular diseases and diabetes are among the leading causes of ill health and premature mortality in Europe. Both conditions are largely preventable, but prevention requires timely data on risk factors and approaches that are accessible to different population groups. Traditional screening methods can be resource‑intensive and may not reach everyone equally.
The researchers reviewed existing evidence on non-clinical measurement methods, such as dried blood spot samples, finger‑prick capillary blood collection, and emerging non‑invasive technologies. Some of these approaches showed close agreement with standard venous blood tests for specific measurements, particularly glycated haemoglobin (HbA1c) and triglycerides.
Clinical standards remain essential
However, the review also makes clear that clinical standards remain essential. Accuracy varies between methods, and differences in sample collection, handling and analysis can affect results. For this reason, self-measurement tools cannot currently replace clinical screening and are not recommended for diagnostic or population-level screening purposes.
“Self-measurement technologies have clear potential to support prevention and reduce barriers to participation,” says researcher (PhD candidate) Hanna Elonheimo, lead author of the study. “At the same time, they should be seen as complementary tools, not alternatives to clinically validated methods.”
The authors highlight that accessible and user‑friendly measurement approaches may still play an important role in increasing awareness of cardiovascular and diabetes risk, supporting disease management, and informing future prevention strategies. Further research is needed to improve standardisation, reliability and regulatory validation before wider implementation can be considered.
Publication: Innovative approaches to early detection of cardiovascular disease and diabetes risk: focus on glucose and cholesterol measuring
Authors: Hanna M Elonheimo, Alexandra Cucu, Gabriela Cristisor, Ciprian Ursu, Claudia Dima, Petru Milos, Giulia Franceschini, Katiuscia Dibiagio, Roberta Papa, Massimiliano Petrelli, Jelka Zaletel, Hanna Tolonen
Journal: European Journal of Public Health
Publication date: 9 February 2026
DOI: https://doi.org/10.1093/eurpub/ckag007
Shaping the EU Safe Hearts Plan: JACARDI joins high-level dialogue on regional and local perspectives
During a high-level discussion bringing together EU and regional stakeholders, JACARDI Coordinator Benedetta Armocida highlighted how coordinated European action can bridge research, policy, and implementation in advancing the EU Safe Hearts Plan. The meeting aimed to explore how regional and local authorities can contribute to shaping and implementing the plan, bringing forward territorial perspectives and feeding into the upcoming Committee of the Regions opinion.
On 6 May 2026, the Interregional Group on Health and Well-being of the European Committee of the Regions, with the support of EUREGHA, hosted the high-level discussion “Shaping the EU Safe Hearts Plan: regional perspectives for cardiovascular health” in Brussels.
The meeting brought together representatives from EU institutions, regional and local authorities, healthcare professionals, researchers, and public health stakeholders to discuss how to advance the implementation of the Safe Hearts Plan (SHP) through stronger multilevel governance and regional action. JACARDI contributed to the discussion as a key European initiative in this field to support the objectives of the SHP.
Cardiovascular diseases remain the leading cause of death and disability in Europe, placing a major burden on individuals, health systems, and economies. Against this backdrop, the discussion highlighted the importance of translating European policy ambitions into concrete and equitable actions adapted to regional and local realities.
Speakers included:
- Carmine Pacente, European Committee of the Regions
- Romana Jerković, European Parliament
- Marianne Takki, European Commission
- Benedetta Armocida, Istituto Superiore di Sanità and Coordinator of JACARDI
- Cristina Gavina, Portuguese Society of Cardiology and European Society of Cardiology
- Antonio Aurigemma, Regione Lazio
The discussion underscored several priorities for the future implementation of the SHP, including strengthening prevention and health promotion, improving early detection and screening, ensuring continuity and integration of care pathways, and addressing persistent inequalities in cardiovascular outcomes, including the cardiovascular gender gap, across and within European regions.
Evidence-informed policies and prevention beyond healthcare settings
Participants also highlighted the growing importance of data systems and digital innovation in supporting evidence-informed and more equitable cardiovascular health policies. At the same time, speakers stressed that effective prevention strategies must extend beyond healthcare settings and reach people directly within schools, workplaces, and local communities, especially underserved populations and people living in vulnerable situations.

Coordinated European action through JACARDI
In this context, Benedetta Armocida presented JACARDI as a concrete example of how coordinated European action can support the objectives of the Safe Hearts Plan by bridging research, policy, and implementation. The Joint Action contributes to strengthening national and regional capacities, fostering collaboration across health systems, and reducing fragmentation in the prevention and management of cardiovascular diseases and diabetes. The discussion concluded with a shared recognition that achieving the ambitions of the EU Safe Hearts Plan will require sustained collaboration between EU, national, regional, and local actors, alongside continued investment in prevention, integrated care, and equity.
The meeting further demonstrated the added value of creating spaces for dialogue between policymakers, researchers, healthcare professionals, and implementers. Bringing together actors operating at different governance levels allows for the exchange of practical experiences, the identification of shared challenges, and the co-development of solutions that are both evidence-based and feasible in real-world settings. Such multistakeholder engagement is essential to ensure that European strategies are translated into sustainable and impactful actions at the regional and local level.
Building stronger prevention systems in Ukraine: insights from the Kyiv JACARDI meeting
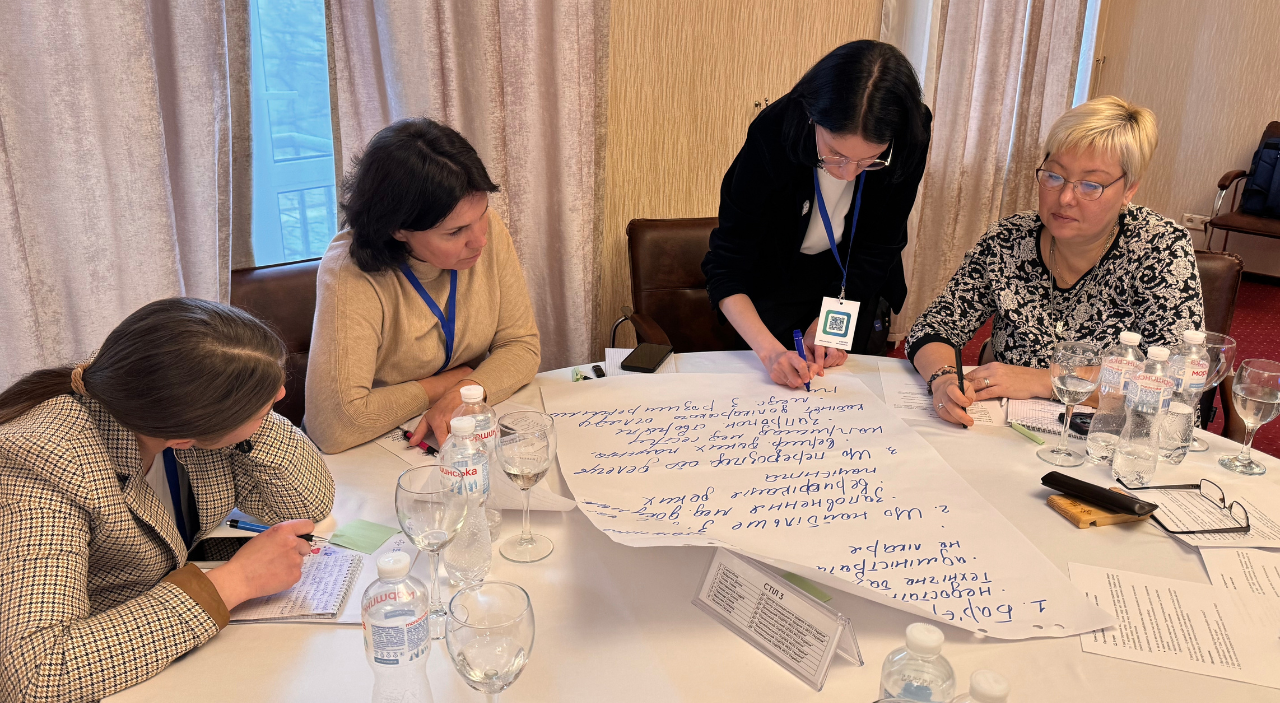
A strategic meeting on implementing effective models for the prevention of cardiovascular diseases and type 2 diabetes was held in Kyiv, Ukraine, organized by the Public Health Center of the Ministry of Health of Ukraine within the framework of JACARDI. The event brought together representatives from the Ministry of Health of Ukraine, the WHO Country Office in Ukraine, and regional centers for disease control and prevention. The main goal of the meeting was to strengthen collaboration in public health, exchange experiences, and integrate European best practices into the prevention of non-communicable diseases (NCDs).
Early identification of risk factors, modern community-level screening models, and international experience in prevention programs were at the forefront of discussions, with special attention on the Safe Hearts Plan. Behavioural risk factors and their impact on premature mortality and population health loss were also high on the agenda.
“Non-communicable diseases often remain ‘invisible’ — their consequences do not appear immediately. At the same time, it is important to understand that prevention is far cheaper than treatment, and healthy nutrition and physical activity are not about trends but primarily about preserving health,” said Tetiana Skapa, Director of the Public Health Department of the Ministry of Health of Ukraine.
What JACARDI pilot studies reveal about prevention and care
The meeting also included discussion of the main findings from a study on health literacy regarding self-monitoring of arterial hypertension. The study was conducted using the Ophelia (Optimising Health Literacy and Access) process, a co-design approach for developing health literacy actions that is applied across 24 pilot projects within JACARDI’s work package on health literacy. The findings of the study confirmed that health literacy is a key factor in the effective prevention and self-management of high blood pressure, influencing adherence to treatment and regular monitoring. The study also highlighted practical opportunities for improvement, including clearer patient communication, better access to blood pressure monitoring in community settings, stronger patient education and peer support, and more coordinated healthcare delivery.




Results from another JACARDI pilot project exploring the barriers to prevention and screening for type 2 diabetes were presented. The study found that while primary care is trusted and access to diagnosis and medications is generally good, key barriers persist, including limited access to diagnostics, high administrative burden, short consultation times, and low patient awareness and motivation for prevention, alongside contextual challenges related to war, such as stress and disruption of care. Lifestyle change remains the greatest challenge for patients, and structured education and support programmes are largely absent. Overall, the findings highlight the need to strengthen prevention, improve access to essential diagnostics, and expand patient and professional education.
“Participation in the JACARDI project allows Ukraine to align with European best practices in cardiovascular disease and diabetes prevention and provides a strategic framework that guides our local prevention efforts, supports early detection, and helps us implement evidence-based interventions tailored to the Ukrainian context, particularly in the challenging conditions of war,” said Nataliia Hryb, Specialist in Non-communicable Disease Prevention at the Public Health Center of the Ministry of Health of Ukraine and pilot lead from the Ukrainian team.
Importance of a systemic prevention approach
Participants emphasized the importance of a comprehensive approach to NCD prevention, including improving health literacy and implementing screening programs. The national “Health Screening 40+” program, which provides basic examinations for early detection of cardiovascular diseases, diabetes, and mental health issues, was also discussed.
“Behavioral risk factors remain the key determinants of premature mortality and health loss in Ukraine,” noted Dmytro Shushpanov, Head of the Department of Demographic Modeling and Forecasting at the M. Ptukha Institute for Demography and Social Research, NAS of Ukraine. “At the same time, significant territorial disparities persist, especially in rural areas, which requires strengthening preventive measures and adapting programs to local conditions.”
Next steps and further collaboration
Following the meeting, participants outlined the key directions for future work: strengthening and supporting community-based prevention programs, developing screening initiatives, and increasing public health literacy. The strategic meeting provided an important platform for reinforcing partnerships between state institutions, regional centers for disease control and prevention, and international organizations.
Equity Lens: Antiracism is integral to reducing health inequalities
Considering the words we use, the decisions we make, and the attitudes we hold, along with recognising discriminatory practices in everyday healthcare settings, are crucial steps public health professionals can take to address health disparities among ethnic minorities. As part of JACARDI’s Equity Lens series, this article examines differences in treatment and care for ethnic minorities, the importance of building trust, and concrete actions professionals can take to achieve more equitable health outcomes.
Since racism directly affects health outcomes, adopting an antiracist approach is integral to quality care, emphasizes Dr. Najma Yusuf, a medical doctor and an antiracism educator for the JACARDI Masterclass titled “Antiracism is care: Advancing Equity in Healthcare”. It is vital to recognize harmful structures, deconstruct them, and avoid past mistakes, especially in the current political climate.
Understanding structural racism and historical context
Racism in healthcare has been well documented and is rooted in structural issues. Studies show that patients from ethnic minorities may receive different treatment than the majority population. This discrepancy is visible even in common medical tests; for instance, in the case of pulse oximetry, which can lead to significant delays in initiating therapy. Diagnosis and treatment decisions made by healthcare professionals can also be influenced by cultural biases.
Dr. Yusuf shed light on the controversial history of medicine, noting that unethical medical experiments conducted on ethnic minorities were a regular occurrence not too long ago. The enduring effects of this history mean that certain minority groups remain wary of healthcare professionals today. Consequently, building trust must begin from the very start, which requires time.
From race-based to race-conscious medicine
A key concern is that race is still used as a risk factor for disease in health research. This persists despite the fact that it has been well-established that race is a social construct, rather than a biological risk factor.
Dr. Yusuf argued that, instead of relying on biology, race should be defined as a social and power construct. This approach allows practitioners to understand and see the effect that race has on an individual’s health and wellbeing. Moving away from race-based medicine toward race-conscious medicine will eventually lead to the reduction of racial health inequalities.
Five concrete ways to promote active antiracism
Antiracism requires active action, and there are concrete ways to promote it within healthcare and healthcare research. Dr. Yusuf presented five actions that professionals can take:
- Admitting the existence of structural racism
- Having active plans to reduce structural racism
- Meeting patients without prejudice
- Disaggregating data in health research for equity monitoring (by country of birth, language, ethnicity)
- Using participatory approaches involving affected communities
Resources:
- Online course on anti-racism for professionals (videos are in Finnish with English subtitles)
- The Moni Suomi Study
- Pulling at the heart: COVID-19, race/ethnicity and ongoing disparities by Chin-Hong, P et al.
- From race-based to race-conscious medicine: how anti-racist uprisings call us to act
- Tackling structural racism and ethnicity-based discrimination in health
About Dr. Najma Yusuf
As a physician specializing in emergency medicine, and an anti-racism expert at the University of Helsinki, Dr. Yusuf has a demonstrated history of working in healthcare, biomedical sciences, and public health. Beyond her medical practice, she is actively engaged in advancing equity and inclusion, serving as a Board Member of the Finnish-Somalia Association (FSA) and as a trainer for doctors in Finland, contributing to a JACARDI pilot program developing antiracist training for healthcare professionals.
About the JACARDI Equity Lens Series:
Throughout this series, we share why equity and diversity are not optional add-ons but core components of truly equitable healthcare as well as a shared responsibility for everyone working in the field. To share the knowledge generated within JACARDI, the Equity Lens article series draws on the JACARDI Equity Masterclass series that provides an in-depth look into matters related to equity and diversity for JACARDI pilot teams conducting 143 healthcare interventions across Europe. The article series offers insights shared by a diverse pool of public health professionals within the consortium. By looking through an equity lens, we can build a more inclusive system for everyone. Join us in learning how an equity lens can shape daily practice and drive meaningful change.
Read the first article in the series: JACARDI’s 4Cs framework for advancing equity and diversity
From pilots to policy: highlights from the Irish JACARDI Heart Health Symposium
The Irish JACARDI Heart Health Symposium took place on 13 February at University College Dublin, bringing together clinicians, researchers, policymakers and programme leads from across Europe. The day showcased the strength of collaboration under JACARDI and the practical progress being made in cardiovascular and diabetes prevention.
The symposium opened with a welcome from Ireland’s Minister for Health, Jennifer Carroll MacNeill, setting the tone of innovation and equity in cardiovascular and diabetes prevention. Dr Benedetta Armocida, Coordinator of JACARDI, provided an overview of JACARDI’s objectives, highlighting the Joint Action’s commitment to shared learning and scalable implementation across Member States.
The spotlight then turned to the pilots – the core of JACARDI. Six pilots from Ireland, Finland, Belgium, Hungary and Ukraine presented their work, with a particular focus on cardiovascular screening and patient self-management.
Pilot presentations: progress across Europe
-
Ireland:
- STOP‑CVD (HSE): Katie Ellwood and Pooja Salgar outlined progress using natriuretic peptide screening to support risk stratification in primary care.
- Healthy Heart Clubs (Croí Heart & Stroke Charity): Lisa Hynes highlighted the importance of structured rehabilitation and long‑term self‑management after cardiac events.
- Finland: Mia Färm (Finnish Diabetes Association) presented the Finnish Risk Calculator, supporting early identification and timely lifestyle intervention.
- Belgium: William Leysen (Diabetes Liga) shared preliminary results from the Halt2Diabetes studies, demonstrating the value of coordinated community‑level screening.
- Hungary: Gréta Máto (OKFŐ) discussed the role of advanced nurse practitioners in strengthening cardiovascular and diabetes screening in primary care.
- Ukraine: Nataliia Hryb (Public Health Centre Ukraine) discussed how they are delivering type 2 diabetes screening in challenging circumstances, underscoring resilience and commitment to patient care.
Across all pilots, a clear message emerged: prevention must be systematic, data-informed and patient-centred.

Women and cardiovascular health: advancing equity
The mid-morning session turned the focus on women with cardiovascular disease (CVD), a key pillar of JACARDI’s commitment to equity and diversity in cardiovascular and diabetes care. The session featured a keynote from JACARDI’s own Dr Héctor Bueno, Co-Leader on the Work Package on Data, who delivered a powerful message: “women are not small men”. His presentation emphasised the need to recognise sex-specific differences in disease presentation, diagnosis, and management.

This was further explored by Dr Mary Ryder, Associate Professor of General Nursing, and Prof. Amy O’Higgins, Consultant Obstetrician at The Coombe Hospital, offering complementary perspectives. Dr Ryder discussed the importance of addressing social determinants of health in cardiovascular prevention, while Prof O’Higgins focused on optimising cardiovascular health during pregnancy, a critical window for long‑term outcomes.
The session was rounded out by a patient story, providing a personal perspective on living with CVD. Her experiences reinforced the human impact behind the statistics and research, leaving a lasting impression on all attendees.
Diabetes and cardiovascular health
The afternoon session turned to diabetes, reflecting its deep interconnection with cardiovascular disease. Dr James (Jim) Januzzi from Harvard Medical School delivered a keynote on heart failure risk across the spectrum of dysglycaemia, stressing the need for integrated approaches. Dr Lisa Devine outlined the successes of Ireland’s Chronic Disease Management Programme, demonstrating how structured, national-level programmes can support early detection, patient engagement, and improved outcomes.
Finally, Prof. Sean Dinneen discussed progress toward a National Diabetes Registry in Ireland, reinforcing the importance of robust data to ensure interventions reach those who need them most, and highlighted the synergies brought about by projects such as JACARDI.
People at the heart of prevention
One of the strongest impressions from the day was how much can be achieved when expertise, curiosity, and compassion are translated into structured action. The symposium wasn’t just about data, tools, or programmes. It was about people: the teams working on the ground across Europe translating strategy into practice, the patients whose stories remind us why these efforts matter, and the exchange of knowledge among colleagues united in a common purpose.
The symposium left attendees not only informed but inspired. It reaffirmed the importance of integrated, patient-centred approaches for a healthier and stronger Europe.
Cardiovascular health in focus: new OECD report and JACARDI experts highlight the path from data to implementation
Cardiovascular disease (CVD) still causes around 1.7 million deaths every year in the European Union. It remains a leading cause of mortality, although most of this burden is preventable. That was the key message of the OECD webinar on 10 February presenting the new EU-funded report ‘State of Cardiovascular Health in the European Union’, which also introduced new monitoring tools and highlighted how the EU Safe Hearts Plan can be translated into practical action, with JACARDI playing an active implementation role.
The webinar, moderated by Francesca Colombo, Head of the Health Division at the OECD Directorate for Employment, Labour and Social Affairs, brought together more than 300 participants from EU institutions, national authorities, research, clinical practice and patient organisations.
Opening the event, Antonio Parenti from the European Commission’s Directorate-General for Health and Food Safety warned that progress in reducing cardiovascular deaths has slowed across Europe. Without stronger prevention and earlier intervention, the overall burden could grow substantially. The recently launched EU Safe Hearts Plan is designed to support Member States in strengthening national plans across prevention, screening, treatment and rehabilitation, with particular attention to vulnerable groups and inequalities in access to care.
New OECD data presented during the webinar show that over three-quarters of cardiovascular deaths in the EU are linked to modifiable risk factors, and trends are worsening in several areas. Around 22% of EU residents live with hypertension, 15% with obesity and 8% with diabetes, while psychosocial risks such as stress, depression and sleep problems affect roughly one third of the population.

Important screening gaps persist: in the 45–54 age group, nearly three in ten adults have not had their blood pressure checked in the past year, and many have gone five years without testing blood sugar or cholesterol. Speakers stressed that screening only improves outcomes when it is followed by timely diagnosis, treatment and long-term patient support.
From the patient perspective, the panel highlighted that delays and fragmentation in diagnosis and care pathways remain a major barrier to better cardiovascular outcomes. Konstantina Boumaki, Board Member of the European Patients’ Forum, warned that late diagnosis and long waiting times not only worsen prognosis but also erode patient trust in the system. She stressed that reducing inequalities is not about delivering identical care to everyone, but about ensuring that all patients can truly access timely diagnosis, treatment and support; a principle that should guide how national cardiovascular plans are designed and implemented.
Alongside the report, the OECD and the European Commission launched a new Cardiovascular Health Dashboard, an online platform that allows policymakers, researchers and the public to track risk factors, care quality and patient pathways across EU countries.
From measurement to implementation
The discussion focused on a recurring weak point in public health policy: implementation. While the evidence on cardiovascular prevention and care is strong, most strategies fail in execution, noted Dr Héctor Bueno, co-leader of JACARDI’s Work Package on data and scientific coordinator of the Cardiovascular Health Strategy of Spain’s National Health System. The key is a clear vision, participation of patients and citizens, as well as political ownership.
Plans only deliver results when they are operational, measurable and realistic, stressed Dr Bueno. Measurement “is essential for visibility and accountability: without indicators, progress cannot be tracked”.
He described how the Spanish strategy is built on a broad indicator framework covering prevention, primary care, acute and chronic care, gender aspects and education, supported by a core set of priority measures. Digital integration, interoperable registries and automated data systems are critical to make monitoring sustainable. Dr Bueno also underlined that aligning scientific evidence, political commitment and citizen engagement is as important as funding when moving from strategy to practice.
JACARDI’s cross-sector contribution to the Safe Hearts Plan
Dr Benedetta Armocida, coordinator of JACARDI, highlighted how the joint action supports the Safe Hearts Plan through cross-sector and patient-journey approaches that connect health literacy, risk awareness, screening and prevention with long-term care pathways. “Cardiovascular prevention is not only a health system responsibility but a societal one, requiring coordinated action across sectors,” Dr Armocida noted, reflecting a Health in All Policies approach.
JACARDI pilots already include early-life interventions to improve children’s understanding of cardiovascular risk and workplace-focused prevention models, alongside broader work on food literacy, healthy environments and equitable access. Digital health and AI tools can accelerate impact, she added, “but only if they are properly integrated into routine care, trusted by users and supported through professional training”.
The overall conclusion was clear: Europe now has stronger data, shared metrics and a dedicated policy framework through the Safe Hearts Plan. With its indicator frameworks, cross-sector pilots and implementation focus, JACARDI is helping to transform evidence and ambition into tangible improvements in cardiovascular health.
References:
OECD (2025), The State of Cardiovascular Health in the European Union, OECD Publishing, Paris
EU Safe Hearts Plan (pdf)
The State of Cardiovascular Health in Europe Dashboard, OECD
The Cardiovascular Health Strategy (CVHS) of Spain’s National Health System, Ministry of Health, Spain (pdf)
Call for papers: join the scientific debate on cardiovascular disease and diabetes
The current policy landscape offers unique momentum for strengthening collective action on noncommunicable diseases. To stimulate discussion on the challenges and opportunities related to cardiovascular disease and diabetes, the International Journal of Public Health and Public Health Reviews have opened a joint call for papers.
Authors are invited to submit Original Articles, Theory and Concept papers, Reviews, and Policy Briefs for the special issue “Strengthening the public health response to cardiovascular diseases and diabetes”. The call for papers is open until 15 January 2027. Submissions will be reviewed by an editorial board that includes two experts from JACARDI, Yhasmine Hamu and Edwin Wouters.
Developed in line with the JACARDI mission, the special issue seeks to foster actionable knowledge that advances effective, equitable, and sustainable responses. Its aim is to support healthier lives, more resilient health systems, and stronger commitment to tackling noncommunicable diseases.
Topics of interest, identified in collaboration with JACARDI, include:
- Primary prevention, including health literacy, awareness, and health promotion
- Screening of high-risk populations
- Integrated health pathways, including health care organization, patient self-management, and reintegration into the workforce
- Data infrastructure and digital technologies as drivers of evidence-informed decision-making and innovation
- Health system strengthening, with a focus on governance, financing, and service delivery
- Strategies to reduce health inequities and ensure that populations living in vulnerable situations are not left behind
Accepted papers will be published on a rolling basis in the online special issue.
Be part of the call and support the creation and dissemination of knowledge that strengthens our public health response to cardiovascular disease and diabetes!
For more information on the call visit the website of the International Journal of Public Health.
How JACARDI can support the implementation of the EU Safe Hearts Plan
Benedetta Armocida, coordinator of JACARDI, presented the Joint Action’s role in shaping screening and early detection approaches under the Safe Hearts Plan, during a dedicated webinar organized by the European Commission.
On 15 January 2026, the European Commission hosted the first stakeholder webinar dedicated to the Safe Hearts Plan, the EU’s first-ever cardiovascular health plan, adopted on 16 December 2025. The online event brought together nearly 500 stakeholders from across Europe and provided a key platform to exchange views on how to support the implementation of the Plan and its flagship initiatives [1].
The webinar [2] marked an important milestone in the roll-out of the Safe Hearts Plan, which aims to tackle cardiovascular diseases (CVDs), the leading cause of mortality in the European Union, through coordinated action on prevention, early detection and screening, and treatment, care and rehabilitation, while addressing cross-cutting challenges such as data and digitalisation, research and innovation, and health inequalities.
Opening the meeting, Commissioner for Health and Animal Welfare, Olivér Várhelyi, underlined the urgency of action and the importance of collaboration with stakeholders to turn the Plan into concrete results.
“Cardiovascular diseases remain Europe’s number one killer, placing a growing burden on our health systems, societies and economies. With the Safe Hearts Plan, we now have a strong policy tool at EU level, but its success will depend on close cooperation with Member States and stakeholders to make it a reality,” said Commissioner Várhelyi.

Supporting early detection and screening
During the webinar, the coordinators of key Joint Actions, JACARDI and JA PreventNCD, presented how their work contributes to the implementation of the Safe Hearts Plan. Dr Benedetta Armocida, coordinator of JACARDI, highlighted the Joint Action’s strong alignment with Pillar 2 of the Plan: early detection and screening, including the flagship initiative on an EU Protocol on Health Checks for CVDs.
JACARDI brings together 21 countries and 81 partners, working to translate EU priorities into concrete, country-level implementation. In particular, Work Package 8 on screening high-risk populations, led by Hanna Tolonen and Luigi Palmieri, is developing common protocols and tools to support Member States in the design, organisation and sustainability of effective screening programmes.
“We are testing and implementing practical solutions that can support the Safe Hearts Plan on the ground. Our pilot projects on early detection and screening aim to generate evidence and tools that help Member States reach high-risk populations, while embedding equity and sustainability across all activities. The aim is to provide further evidence and the result of our pilots to support the implementation of the European plan,” said Dr Armocida.
In practice, JACARDI is implementing 19 pilot projects focused on screening for CVDs and diabetes across different European countries, assessing the feasibility of diverse screening approaches. The Joint Action has also developed an online risk assessment tool selection guide, supporting professionals in selecting appropriate risk prediction methods.
Addressing inequalities is a core priority for JACARDI, fully aligned with the Safe Hearts Plan. Across its 143 pilot projects, the Joint Action promotes equity and diversity, targeting both the general population and high-risk groups, with a focus on integrated care pathways, self-management and social participation.
The webinar also showcased the strong alignment between the Safe Hearts Plan and other EU initiatives. Knut Jønsrud, project manager of JA PreventNCD, emphasised the importance of addressing key risk factors and reducing social inequalities through a life-course approach.
“Several flagship initiatives of the Safe Hearts Plan, such as modernising tobacco control legislation and strengthening health literacy, are closely aligned with our work. A people-centred, equity-focused approach and cross-sectoral collaboration are essential to achieving lasting impact,” said Jønsrud.
A coordinated EU response
Antonio Parenti, director for Public Health, Cancer and Human Security in the Directorate General for Human and Food Security of the European Commission (DG SANTE), stressed the scale of the challenge posed by CVDs and the need for decisive, coordinated action at EU level.
“CVDs cost the EU more than €280 billion every year. Without strong and coordinated action, this burden will continue to grow, affecting future generations, health systems and economic resilience. The Safe Hearts Plan is our collective response to this challenge,” Parenti stated.
He highlighted the Plan’s three pillars and its ten flagship initiatives, designed to improve population health, foster innovation and support sustainable healthcare systems. Prevention remains a cornerstone of the Plan, as nearly 80% of CVDs can be prevented through lifestyle changes, alongside strengthened, patient-centred and multidisciplinary care [3].
Next steps
The European Commission will now collect and analyse the feedback and ideas shared by stakeholders during the webinar. A second stakeholder webinar is planned for the second half of 2026, ensuring continued dialogue as the Safe Hearts Plan moves into its implementation phase.
For JACARDI, the webinar confirmed the relevance of Joint Actions as key instruments to support EU health policies and demonstrated how collaborative, evidence-based approaches can help reduce the burden of CVDs across Europe.
[1] About the Safe Hearts Plan flagship initiatives
Adopted in December 2025, the EU Safe Hearts Plan is underpinned by ten flagship initiatives designed to deliver clear EU added value across prevention, care and innovation, while supporting Member States in addressing cardiovascular diseases in a coordinated and sustainable way:d
- A lifelong, personalised and digitally enabled prevention programme – ‘EU cares for your heart’
- Empowering consumers through information on food processing in the EU
- Modernising tobacco control legislation
- The Commission will examine which appropriate tools, including possible financial actions, could be deployed to support/fund public health actions in the field of primary prevention and stimulate food reformulation and healthier consumer choices
- Proposal for a Council recommendation on vaccination against respiratory infections as a preventive measure for cardiovascular diseases
- EU protocol on health checks for cardiovascular diseases
- Proposal for a Council recommendation on personalised treatment and monitoring of cardiovascular diseases
- Incubator for innovation and integration of AI and digital technologies in cardiovascular healthcare
- EU cardiovascular health inequalities dashboard
- Cardiovascular Disease Research and Innovation Roadmap
[2] Stakeholder Webinar the Safe Hearts Plan – Meeting documents
[3] Questions and answers on the EU Safe Hearts Plan
A defining CVH moment in Europe: The Commission announced the Safe Hearts Plan
“When Europe acts together, we do not simply improve systems, we improve lives,” points out Benedetta Armocida, Coordinator of JACARDI, as the European Union’s Cardiovascular Health Plan is launched. At a time when cardiovascular disease remains Europe’s leading cause of death, this moment marks a collective step toward strengthening heart health across the continent.
Cardiovascular diseases (CVDs) remain the leading cause of death and disability in Europe, as confirmed by the newly released OECD report “The State of Cardiovascular Health in the European Union“. CVD claims 1.7 million lives each year, more than cancer and diabetes combined, and affects an estimated 62 million people. CVDs also contribute significantly to disability, early retirement, and absenteeism, lower the quality of life and reduce life expectancy, according to data from the European Commission [1], [2], [3].
The total economic burden of CVD in the EU is estimated at EUR 282 billion annually, around 2% of GDP, and significantly higher than that of cancer. The OECD report highlights stark geographic, gender and socio-economic disparities in cardiovascular outcomes and access to care, reinforcing the need for coordinated EU-level action. It also acknowledges JACARDI’s input to the report, and references JACARDI’s 4C Framework and pilot actions in France and Spain.
Bearing that in mind, the European Commission’s launch of the Cardiovascular Health Plan, under the name Safe Hearts Plan, marks a decisive moment for public health in the region. JACARDI strongly welcomes this Plan, as coordinated European action is essential to reduce the number of people falling ill with cardiovascular diseases, and to prevent premature deaths for those with existing conditions or risk factors, such as obesity, diabetes and high blood pressure.
“The launch of the Cardiovascular Health Plan marks a pivotal moment for Europe’s public health. JACARDI welcomes this initiative, recognizing the crucial role of Joint Actions in fostering collaboration among countries, experts, and stakeholders. By working together, sharing knowledge, and aligning efforts, we can ensure that advances in prevention, care, and innovation in cardiovascular health truly reach all communities, leaving no one behind,” notes Prof Graziano Onder, Scientific Coordinator of JACARDI.
The Plan arrives at a critical time. For too long, CVD and diabetes have lacked the political visibility their burden demands. The CVH Plan opens the door to a new European approach that puts prevention first, strengthens early detection and screening, and promotes equity and integrated, patient-centred care across health systems. For JACARDI, this initiative is an essential step towards making the healthy choice the easy and default choice for citizens across Europe.
“The CVH Plan is a decisive step forward, and JACARDI is proud to contribute with its experience and technical expertise. Our work shows that no cardiovascular strategy can be effective without putting equity at the centre, addressing the gaps linked to income, geography, education and gender that still shape health outcomes across Europe. We look forward to supporting the implementation of a Plan that has the potential to change lives across the region”, explains Dr Benedetta Armocida, coordinator of JACARDI.
The CVH Plan is needed as fragmented efforts can no longer address challenges that are inherently interconnected. “Prevention, early detection, treatment, rehabilitation, digital innovation, community engagement, these elements only create real impact when they are aligned and mutually reinforcing”, adds Dr Armocida.
Equally important is the improvement of data collection and use, ensuring that high-quality, reliable information drives policy decisions, guides clinical practice and allows progress to be measured transparently across countries, as highlighted in a recent policy paper published in The Lancet Regional Health – Europe, developed jointly by the Joint Action on Cardiovascular Diseases and Diabetes (JACARDI), the Joint Action Prevent Non-Communicable Diseases (JA PreventNCD), and the WHO Regional Office for Europe (WHO/Europe), [4].
“Robust and accessible data are essential to understand where inequalities arise, to identify people at risk earlier and to ensure timely, high-quality care across Europe. Strengthening data systems, from availability and quality to interoperability and sharing, is key to improving early detection, screening programmes and continuity of care”, says Dr Héctor Bueno, co-leader of the working group on data availability, quality, accessibility and sharing from JACARDI.
Through its multidisciplinary network, technical expertise and strong partnerships, JACARDI stands ready to support the successful rollout of the Safe Hearts Plan. The Joint Action will continue to contribute practical knowledge on prevention, governance, data systems and quality of care, building on lessons learned from other European health initiatives and aligning closely with the shared vision set out by the European cardiovascular community.
Joint Actions are more than projects, they are engines of collaboration. JACARDI can serve as a bridge between countries, stakeholders, and other EU initiatives, helping to translate the CVH Plan into coordinated, coherent, and sustainable action across Europe.
JACARDI is generating concrete insights on equity, early detection, integrated care, digital tools, data systems, and workforce capacity. These lessons, grounded in practice and validated across diverse health systems, can inform the plan’s priorities, standards, and operational frameworks. JACARDI remains fully committed to supporting the European Commission in prioritizing the Cardiovascular Health Plan and promoting its effective implementation across Member States, ensuring that every step forward translates into meaningful impact for people’s health.
The Safe Hearts Plan at a glance:
• Prioritises prevention as one of its main pillars
• Sets clear targets, including reducing mortality related to cardiovascular disease by 25% by 2035
• Encourages Member States to develop or implement national cardiovascular health plans by 2027
• Emphasises reducing health inequalities and improving access to healthcare
• Supports an EU protocol on health checks to shift the focus from treatment to prevention
• Addresses lifestyle risks, including unhealthy diets, ultra-processed foods, and smoking
Read the full European Commission Safe Hearts Plan here.
References:
[1] OECD (2025), The State of Cardiovascular Health in the European Union, OECD Publishing, Paris,
[2] Cardiovascular health; European Commission
[3] Fighting cardiovascular disease – a blueprint for EU action, June 2020. European Heart Network and the European Society of Cardiology.
[4] Benedetta Armocida, Hanna Tolonen, Ivo Rakovac, Beatrice Formenti, Jill Farrington, Allison Ekberg, Hector Bueno, Giovanni Capelli, Silvia Francisci, Morten S. Frydensberg, Ane Fullaondo, Linda Granlund, Yhasmine Hamu Azcarate, Torben F. Hansen, Emil Høstrup, Tomi Mäki-Opas, Luigi Palmieri, Markku Peltonen, Valentina Possenti, Marco Silano, Gundo Weiler, Kremlin Wickramasinghe, Edwin Wouters, Knut-Inge Klepp, Graziano Onder, Gauden Galea, Strengthening non-communicable diseases monitoring systems in Europe through a multistakeholder collaborative approach: a key priority for advancing data-driven policymaking, The Lancet Regional Health – Europe, Volume 61, 2026, 101553, ISSN 2666-7762,
JACARDI’s synergies with Action Grants: reducing the cardiovascular burden together
The five Action Grants – CaregIVR, PERFECTO, Preventia, PROVIDE, RESIL-Card – and JACARDI are all anchored in the urgent mission of tackling the burden of cardiovascular diseases (CVD), Europe’s leading cause of death, which is especially timely as the European Commission develops the European Cardiovascular Health Plan (CVH Plan). This partnership is built upon the understanding that up to 80% of premature CVD deaths are preventable, and aims to strengthen cohesive EU-level action.
The overarching goal uniting JACARDI and these projects is the comprehensive reduction of the immense public health burden caused by Non-Communicable Diseases (NCDs), particularly Cardiovascular Diseases (CVD) and diabetes. This is pursued through a shared commitment to developing and promoting the implementation of validated best practices throughout the entire patient journey.
Within the implementation domain, projects focused on early detection, such as PERFECTO and PROVIDE, are collaborating with JACARDI WP8 to develop standardized screening protocols. Addressing health system continuity, RESIL-Card partners with JACARDI WP9 to specifically build resilience in cardiovascular care pathways, ensuring high-quality care continuity during crises.
Key expected outcomes include strengthening patient-centered approaches, utilizing novel digital tools like predictive algorithms by PROVIDE and immersive technology by CaregIVR, and developing tools such as the resilience assessment toolkit by RESIL-Card.
Synergies around equity are strengthened by sharing JACARDI’s “4Cs” Framework, which helps projects like CaregIVR and Preventia ensure targeted outreach to vulnerable populations. Both Preventia and PROVIDE showcase the central role of innovative digital tools in prevention efforts.
By coordinating our approach across technical work packages among these projects, we maximize collective impact and ensure that project outcomes translate effectively into actionable policy, creating roadmaps that support the scaling up of experiences at the national and regional levels.Ultimately, this unified collaboration contributes to promoting prevention, early detection, education, and sustained behavioral change for a healthier future.